Download
1 / 30
320 likes | 406 Vues
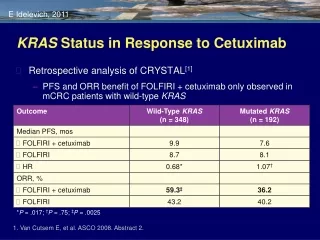
Analysis of CRYSTAL study shows better outcomes in KRAS wild-type patients receiving FOLFIRI + cetuximab for mCRC treatment. Study demonstrated increased ORR, longer PFS, and higher resection rates in KRAS wild-type population. Safety profile was as expected for combined therapy.

E N D
KRAS Status in Response to Cetuximab Retrospective analysis of CRYSTAL[1] PFS and ORR benefit of FOLFIRI + cetuximab only observed in mCRC patients with wild-type KRAS E Idelevich, 2011 *P = .017; †P = .75; ‡P = .0025 1. Van Cutsem E, et al. ASCO 2008. Abstract 2.
20060314FOLFIRI + Panitumumab in 1st-line Treatment of Metastatic CRC E Idelevich, 2011 S c r e e n I n g E n r o l l m e n t Endoftreatment S a f e t yf ollowup Endofs t u d y FOLFIRI (Q2W) +panitumumab 6 mg/kg(Q2W, on day 1 of each cycle) Metastatic CRC (n=150) Approx. 56 daysafter end of treatment • Study objectives: To estimate the effect of KRAS mutation status on efficacy and to describe the safety profile • Study endpoints: ORR (1°); PFS, Safety Köhne CH, et al. ASCO-GI 2010, #414, poster presentation; www.amgentrials.com; protocol ID: 20060314. ClinicalTrials.gov identifier: NCT00508404.
20060314Best Objective Response E Idelevich, 2011 Köhne CH, et al. ASCO-GI 2010, #414, poster presentation.
Resection Rates – Patients with Liver Only Disease E Idelevich, 2011 20060314 Overall resections 40 KRAS evaluable 35 Resection rate (%) 20 13 0 KRAS wt (n=11/31) KRAS mt (n=2/16) Hofheinz R, et al. ASCO 2010, #3545, poster presentation
20060314Progression-free Survival Primary Analysis Set 100 90 80 70 60 50 40 30 20 10 0 EIdelevich, 2011 HR = 0.46 (95%CI: 0.31–0.70) Proportion Event-Free (%) 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 Months Köhne CH, et al. ASCO-GI 2010, #414, poster presentation.
20060314Summary This was the first study to investigate the effect of tumour KRAS status on response to panitumumab plus FOLFIRI in the 1st-line treatment of mCRC KRAS wt tumours were more likely to respond to treatment with panitumumab plus FOLFIRI (56.5%vs 37.9%) PFS was longer in patients with KRAS wt tumours Resection rate was higher in the KRAS wt population Safety was as expected for an anti-EGFR inhibitor plus irinotecan-based chemotherapy in this setting E Idelevich, 2011 Köhne CH, et al. ASCO-GI 2010, #414, poster presentation; Hofheinz R, et al. J Clin Oncol 2010; 28(15S): #3545, poster presentation.
20050181FOLFIRI ± Panitumumab in 2nd-line Treatment of Metastatic CRC E Idelevich, 2011 Longtermf ollowup Endoftreatment FOLFIRI (Q2W) +panitumumab 6 mg/kg(Q2W) Metastatic CRC (n=1100) R FOLFIRI (Q2W) 1:1 Disease assessment every 8 weeks • Stratification by: • ECOG score: 0-1 vs. 2 • Prior oxaliplatin exposure for mCRC • Prior bevacizumab exposure for mCRC • Study endpoints: PFS/OS (co-1°); ORR, Safety, PRO PRO, patient-reported outcomes Peeters M, et al. J Clin Oncol 2010;28:4706-4713;ClinicalTrials.gov identifier: NCT00339183; www.amgentrials.com; protocol ID: 20050181.
20050181Objective Response in Patients with KRAS wt Tumours (Central Review) E Idelevich, 2011 40 30 35 Objective Response Rate (%) 20 10 10 0 Panitumumab+ FOLFIRI(n=297) FOLFIRI(n=285) • More than 3x as many patients responded to panitumumab p < 0.001(descriptive); All responses were confirmed no earlier than 28 days after the response criteria were first met Peeters M, et al. J Clin Oncol 2010;28:4706-4713.
20050181Panitumumab Improved Median PFS by 51% in Patients with KRAS wt Tumours 0 2 4 6 8 10 12 14 16 18 20 E Idelevich, 2011 1.0 0.9 0.8 0.7 HR = 0.73 (95%CI: 0.59–0.90) p = 0.004 0.6 0.5 Progression-Free Probability 0.4 0.3 0.2 0.1 0.0 Months Peeters M, et al. J Clin Oncol 2010;28:4706-4713.
20050181Summary This is the first randomised studyprospectively analysed byKRAS status in 2nd-line mCRC In patients with KRAS wt tumours, panitumumab significantly improved PFS when added to FOLFIRI Overall survival was numerically improved (not significant) The response rate was improved by more than 3x (35% vs 10%) Safety was as expected for an anti-EGFR antibody in combination with FOLFIRI E Idelevich, 2011 Peeters M, et al. J Clin Oncol 2010;28:4706-4713. Peeters M, et al. ASCO-GI 2010, #282, oral presentation
Metastatic colon cancer patients (100%) Non - resectable 75% Resectable 25% 63% 12% Potentially Down-sizable Non curable
Paul Brousse Experience - 1439 Patients (1988–1999) Adam R et al Ann Surg. 2004;240:644-658
Treatment of Metastatic CRC 1980 1985 1990 1995 2000 2005RR %MS Months 5Fu 20-25 13 Capecitabine Irinotecan 40- 50 20-22 Oxaliplatin EGFR inhibitors ~ 60 > 24 Bevacizumab
Endpoints for assessment of systemic therapy for potentially resectable disease • Systemic therapy is enabling resection -Highest RR maximizes resection rate(Folprecht et al) • Endpoints - PFS is primary efficacy endpoint(ECNTG, 2007) - Secondary endpoints * Response Rate * Liver related toxicity * Achievement of R0 resection of all disease Are biological essential? - if acceptable toxicity, higher RR, improved resection rates and ultimately improved PFS are demonstrated (European Journal of Cancer, 43 (2007), 2037-2045)
Response rates: recent phase 3 trials RegimenResponse Rate Reference _________________________________________________________________________ FOLFOX36% NS; FOFOX+cetuximab 46% (OPUS, Bokemeyer) _____________________________________________________________________________________ FOLFIRI43% p=0.004; FOLFIRI+cetuximab 59% (CRYSTAL,van Cutsem) ______________________________________________________________________________________ FOLFOX38% NS; FOLFOX+bevacizzumab 38% (XELOX-1/NO16966 Saltz) ______________________________________________________________________________________ FOLFOX 47% NS; p=0.06 FOLFOX+panitumumab 55 (PRIME, J-Y Douillard) ______________________________________________________________________________________ FOLFIRI36% p=0.001; FOLFOXIRI 60% (Falcone) ______________________________________________________________________________________ FOLFOX+bevacizumab 41% NS; FOLFOX+bevacizumab+cetuximab 39% (PACCE; Hecht) ______________________________________________________________________________________ CAPOX+bevacizumab 44% NS; CAPOX+becizumab+cetuximab 44% (CAIRO2; Punt) ______________________________________________________________________________________ Standard Doublets ~ 40% Response Rate (RR)
Response rates: recent phase 3 trials RegimenResponse Rate Reference ______________________________________________________________________________________ FOLFOX 36% NS; FOFOX+cetuximab 46% (OPUS, Bokemeyer) ______________________________________________________________________________________ FOLFIRI 43% p=0.004; FOLFIRI+cetuximab59%(CRYSTAL,van Cutsem) ______________________________________________________________________________________ FOLFOX 38% NS; FOLFOX+bevacizzumab 38% (XELOX-1/NO16966 Saltz) ______________________________________________________________________________________ FOLFOX 47% NS; p=0.06 FOLFOX+panitumumab 55% (PRIME, J-Y Douillard) ______________________________________________________________________________________ FOLFIRI 36% p=0.001; FOLFOXIRI 60%(Falcone) ______________________________________________________________________________________ FOLFOX+bevacizumab 41% NS; FOLFOX+bevacizumab+cetuximab 39% (PACCE; Hecht) ______________________________________________________________________________________ CAPOX+bevacizumab 44% NS; CAPOX+becizumab+cetuximab 44% (CAIRO2; Punt) ______________________________________________________________________________________ Adding EGFR inhibitors or using triplet chemotherapy increases RR
Response rates: recent phase 3 trials RegimenResponse Rate Reference _____________________________________________________________________________________ FOLFOX 36% NS; FOFOX+cetuximab 46% (OPUS, Bokemeyer) _____________________________________________________________________________________ FOLFIRI 43% p=0.004; FOLFIRI+cetuximab59%(CRYSTAL,van Cutsem) ______________________________________________________________________________________ FOLFOX 38% NS; FOLFOX+bevacizzumab 38% (XELOX-1/NO16966 Saltz) ______________________________________________________________________________________ FOLFOX 47% NS; p=0.06 FOLFOX+panitumumab 55%(PRIME, J-Y Douillard) ______________________________________________________________________________________ FOLFIRI 36% p=0.001; FOLFOXIRI 60%(Falcone) ______________________________________________________________________________________ FOLFOX+bevacizumab 41% NS; FOLFOX+bevacizumab+cetuximab 39% (PACCE; Hecht) ______________________________________________________________________________________ CAPOX+bevacizumab 44% NS; CAPOX+becizumab+cetuximab 44% (CAIRO2; Punt) ______________________________________________________________________________________ Bevacizumab does not increase Response Rate (RR)
Kras-dependent RR in First-Line Trials RR (K-ras w.t.) RR (K-ras mut) __________________________________________________________________ OPUS (Bokemeyer) FOLFOX 37% 49% FOLFOX+erbitux 61% 33% __________________________________________________________________ CRYSTAL(van Cutsem) FOLFIRI43%40% FOLFIRI+erbitux 59% 38% __________________________________________________________________ PRIME(J-Y Douillard) FOLFOX 47% 40% FOLFOX+vectibix55% 40% __________________________________________________________________ 20060314(Köhne CH) FOLFIRI+vectibix56,5% 37.9% __________________________________________________________________
Response Rate • In K-ras wild type patients - FOLFOX or FOLFIRI+EGFR inhibitors has shown 55%- 60% response rate • FOLFOXIRI - 60% response rate in small phase 3 trial
What is the optimal chemotherapy for the neoadjuvant treatment of unresectable liver metastases?
In patients with K-ras unknown or mutant - FOLFOX remains a standard treatment - FOLFOXIRI is an option (resectability, RR + PFS), but unknown toxicity profile in larger series - FOLFOX + bevacizumab is safe, but neither improves response rates nor resection rates • In patients with wildtype K-ras - FOLFOX or FOLFIRI + EGFR inhibitors improve resection rates - FOLFIRI + cetuximab improves resection rate compared FOLFIRI
Treatment of unresectable mCRC • Patients needing or desiring an aggressive approach: - patients with potentially resectable metastases - patients with clearly symptomatic disease in whom tumor regression is needed • KRAS wild type patients: - CT + panitumumab, CT+cetuximab -evidence for response is greater for cetuximab in neoadjuvant approach • KRAS mutant patients: - CT + bevacizumab - FOLFOXIRI may be an option if contraindications for bevacizumab and downsizing is desired Van Cutsem E, et al. WCGIC 2009 Expert Opinion
Treatment of unresectable mCRC Specific issues • Treat with biologicals until progression or toxicity, or until metastases become resectable • Continue treatment until progression with biologicals, even if one of the cytotoxic partners (oxaliplatin, irinotecan) is stopped • No clear evidence to administer biologicals beyond progression • Correlation of rash and activity after anti-EGFR antibodies has no immediate practical implications in clinical practice Van Cutsem E, et al. WCGIC 2009 Expert Opinion
! Non curable Non curable Stage IV Colon Cancer Group I Group II Group III Group IV Curable Potentially Symptomatic Asymptomatic disease curablenon curablenon curable disease disease disease
First line strategy of metastatic CRC Dose the patient need (or desire) aggressive therapy? No ~ 15% Yes ~ 85% K-RAS 5FU/Cape +/- bev + inh.EGFR(WT) Unavailable WT MUT Doublet + bev Doublet + bev Doublet + EGFR inhibitors Doublet + bevacizumab Van Cutsem E, et al. WCGIC 2009 Expert Opinion
Optimal Chemotherapy for the neoadjuvant treatment of non- resectable liver metastases –Do we have to include biologics in this setting? Conversion Therapy Considerations: Practical Management • Role of FOLFOX better established than FOLFIRI - Better toxicity profile, more clinical data • FOLFOXIRI attractive … • Limit duration of pre-operative therapy to 3-4 months - Don’t treat to best response, but to resectability - Decrease hepatotoxicity • Role of biologics is evolving - Bevacizumab is not mandatory! -If Bevacizumab is used, d/c 6 wks before planned surgery • EGFR inhibitors could emerge as best option in K-ras wild type CRC
Take-home Messages Aggressive Multi-disciplinaryApproach
Thank you!