Download
1 / 66
680 likes | 945 Vues
Bacterial Vaginosis, Periodontal Disease and Preterm Birth Eyal Sheiner MD, PhD. Department of Obstetrics and Gynecology, Soroka University Medical Center, Be ’ er-Sheva. BACKGROUND. Preterm birth Major public health issue in the US

E N D
Bacterial Vaginosis, Periodontal Disease and Preterm Birth Eyal Sheiner MD, PhD Department of Obstetrics and Gynecology, Soroka University Medical Center, Be’er-Sheva.
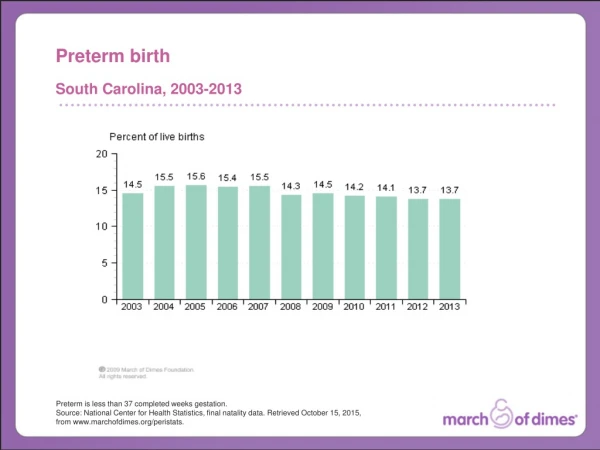
BACKGROUND • Preterm birth • Major public health issue in the US • Account for 75% of perinatal mortality and more than 50% the long-term morbidity Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
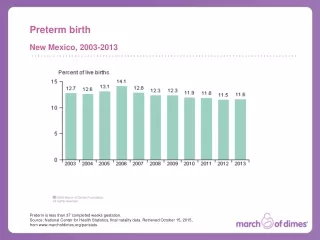
Preterm Birth in the USA Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Obstetric Precursors of PTB Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Temporal Changes Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Infection and PTB • Intrauterine infection- frequent and important mechanism leading to PTB • The mechanisms: activation of the innate immune system • Release of inflammatory chemokines and cytokines (IL-6, IL 8, IL1β, TNF α.) Romero R, Gotsch F, Pineles B, Kusanovic JP. Nutr Rev. 2007 65:S194-202.
Infection and PTB • Microbial endotoxins and proinflammatory cytokines stimulate the production of • Prostaglandins • Inflammatory mediators • Matrix-degrading enzymes • Prostaglandins stimulate uterine contractility, • degradation of extracellular matrix in the fetal membranes leads to PPROM Romero R, Espinoza J, Kusanovic JP, Gotsch F, Hassan S, Erez O, Mazor M. BJOG. 2006 113:17-42.
Infection and PTB • Intrauterine infection might account for 25–40% of PTB Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Potential Routs for Infection Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Potential Routs for Infection Goldenberg RL, Culhane JF, Iams JD, Romero R. Lancet. 2008 5;371(9606):75-84.
Bacterial Vaginosis • Bacterial vaginosis is a clinical syndrome defined by a change in the microbial ecosystem of the vagina • Reduction in the normal lactobacillary bacteria and heavy overgrowth of mixed anaerobic flora: • Gardnerella vaginalis • Mycoplasma hominis • Mobiluncus species Amsel et al. Am J Med. 1983 Jan;74(1):14-22.
Bacterial Vaginosis • Hydrogen peroxide-producing lactobacilli important in preventing overgrowth of anaerobes in normal vaginal flora • Bacterial vaginosis does not appear to be sexually transmitted but may be associated with sexual activity Amsel et al. Am J Med. 1983 Jan;74(1):14-22.
Bacterial Vaginosis • Bacterial vaginosis is often asymptomatic but may result in a vaginal discharge which can be grey in color with a characteristic ’fishy’ odor • It is not associated with vaginal mucosal inflammation and rarely causes vulval itch The Cochrane Library 2009,4
Diagnosis: BV (¾ Criteria) • Diagnosed clinically by the presence of: • Clue cells on Garm stein • Vaginal pH greater than 4.7 • A profuse white homogeneous discharge • A fishy odor when the vaginal discharge is exposed to potassium hydroxide Amsel et al. Am J Med. 1983 Jan;74(1):14-22.
Bacterial Vaginosis • In the laboratory, (Nugent criteria): • Gram-stained smears are scored on the basis of low number of lactobacilli • The presence of high number of organisms resembling mobiluncus • A score of 7–10 diagnostic (1.5-to 3-fold increase in the rate of preterm birth) Nugent et al. J Clin Microbiol. 1991 Feb;29(2):297-301.
Bacterial Vaginosis • Bacterial vaginosis is present in up to 20% of women during pregnancy • The majority will be asymptomatic • May spontaneously resolve without treatment, although most women will have persistent infection later in pregnancy The Cochrane Library 2009,4
Screening for infection The Cochrane Library 2009,4
Screening for infection • Multicentre, prospective, randomized controlled trial • 4155 pregnant women early in the second trimester were screened by Gram stain for asymptomatic vaginal infection • Intervention: standard treatment (clindamycin 2%); control group, the results of the vaginal smears were not revealed to the caregivers Kiss et al. BMJ. 2004 Aug 14;329(7462):371
Screening for infection • In the intervention group, the number of PTB was significantly lower than in the control group (3.0% v 5.3%, 95% CI 1.2 to 3.6; P = 0.0001). Kiss et al. BMJ. 2004 Aug 14;329(7462):371
Screening for infection Integrating a simple infection screening program into routine antenatal care leads to a significant reduction in PTB in a general population of pregnant women Kiss et al. BMJ. 2004 Aug 14;329(7462):371
Bacterial Vaginosis • 10,397 pregnant women from 7 medical centers who had no known medical risk factors for PTB • At 23 to 26 weeks' gestation, BV was determined by vaginal pH and the results of Gram's staining • BV was detected in 16 % Hillier SL et al. N Engl J Med 1995; 333: 1737–42.
Bacterial Vaginosis Hillier SL et al. N Engl J Med 1995; 333: 1737–42.
Bacterial Vaginosis • In a multivariate analysis, the presence of BV was related to preterm delivery of a low-birth-weight infant (OR 1.4; 95% CI 1.1 to 1.8). Hillier SL et al. N Engl J Med 1995; 333: 1737–42.
Bacterial Vaginosis • CONCLUSIONS: Bacterial vaginosis is associated with the PTB & low-birth-weight infants independently of other recognized risk factors Hillier SL et al. N Engl J Med 1995; 333: 1737–42.
Bacterial Vaginosia • To assess the effects of antibiotic treatment of bacterial vaginosis in pregnancy • It was not possible to stratify results into symptomatic vs. asymptomatic BV- symptoms lead to treatment The Cochrane Library 2008,4
Bacterial Vaginosia The Cochrane Library 2009,4
Bacterial Vaginosia The Cochrane Library 2009,4
Bacterial Vaginosia The Cochrane Library 2009,4
Bacterial Vaginosia The Cochrane Library 2009,4
Bacterial Vaginosia The Cochrane Library 2009,4
Bacterial Vaginosia The Cochrane Library 2009,4
Conclusions, Cochrane • Antibiotic treatment can eradicate BV in pregnancy • Little evidence that screening and treating all pregnant women with asymptomatic bacterial vaginosis will prevent PTB and its consequences • Treatment before 20 weeks’ gestation may reduce the risk of PTB The Cochrane Library 2009,4
Conclusions, Williams 23ed • No doubt that adverse vaginal flora is associated in some way with spontaneous PTB • Unfortunately, to date, screening and treatment have not been shown to prevent PTB
Periodontal Disease • Several non-genital tract infections are associated with, and probably predispose to, PTB
J Matern Fetal Neonatal Med 2009 Feb;22(2):124-8 J Matern Fetal Neonatal Med 2009 May;22(5):423-7.
J Matern Fetal Neonatal Med. 2010, in press Am J Perinatol. 2010 in press
What is Periodontal Disease? • Periodontal disease is an oral chronic anaerobic infection caused by bacteria in the plaque on the oral surfaces • These bacteria have the ability to colonize sub-gingival plaque and generate by-products that directly injure tissue and elicit inflammatory or immune responses
What’s the link? • Periodontitis is common, with a reported prevalence of >30% in some populations • There is substantial observational evidence that links maternal periodontal disease to PTB, possibly because of the maternal inflammatory response to periodontal disease Macones et al. Am J Obstet Gynecol 2010 Feb;202(2):147.e1-8.
What’s the link? • The bacteria associated with periodontal disease are capable of stimulating excessive production cytokines and prostaglandins, potentially causing PTB Macones et al. Am J Obstet Gynecol 2010 Feb;202(2):147.e1-8.
Periodontal Disease • Randomized, controlled study comparing preterm births among 4 treatment groups of pregnant women with periodontisis: • Dental prophylaxis + placebo (N=123) • Scaling and root planing + placebo (N=123) • Scaling and root planing+ metronidazole(N=120) • No treatment (N=723) Jeffcoat et al. J Periodontol. 2003 Aug;74(8):1214-8.
Periodontal Disease Jeffcoat et al. J Periodontol. 2003 Aug;74(8):1214-8.
Periodontal Disease • Scaling and root planing in pregnant women with periodontitis may reduce PTB in this population • Adjunctive metronidazole therapy did not improve pregnancy outcome Jeffcoat et al. J Periodontol. 2003 Aug;74(8):1214-8.
Periodontal Disease and PTB Metaanalysis OR=2.83 95% CI 1.95-4.10 Vergnes et al : Am J Obstet Gynecol 2007;196:135.
The data used were not robust enough to recommend screening and treatment of pregnant women • Dental interventions can not be recommended as preventive therapy for PTB based on the research currently available • Further research is needed to better characterize the association to explore the affects of dental therapy on pregnancy outcome
Periodontal Disease and PTB Honest et al. Health Technology Assessment 2009; 13: 43
Periodontal Disease- Metaanalysis • Metaanalysis of RCT to determine whether periodontal disease treatment with scaling and/or root planing during pregnancy may reduce PTB or LBW • Treatment resulted in significantly lower PTB (odds ratio [OR], 0.55; 95% CI, 0.35-0.86; P = .008) and borderline significantly lower LBW (OR, 0.48; 95% CI, 0.23-1.00; P = .049) Polyzos et al. Am J Obstet Gynecol. 2009 Mar;200(3):225-32.
Periodontal Disease- Metaanalysis OR=0.55; 95% CI 0.35-0.86 Polyzos et al. Am J Obstet Gynecol. 2009 Mar;200(3):225-32. Polyzos et al. Am J Obstet Gynecol. 2009 Mar;200(3):225-32.
Periodontal Disease- Metaanalysis • Subgroup analysis suggested significant effect of treatment in: • Absence of history of PTB (OR, 0.48; 95% CI, 0.29-0.77; P = .003) • Less severe periodontal disease as defined by probing depth (OR, 0.49; 95% CI, 0.28-0.87; P = .014) or bleeding on probing site (OR, 0.37; 95% CI, 0.14-0.95; P = .04). Polyzos et al. Am J Obstet Gynecol. 2009 Mar;200(3):225-32.
Periodontal Disease- Metaanalysis • “If ongoing large and well-designed RCT support our results, we might need to reassess current practice or at least be cautious prior to rejecting treatment of periodontal disease with scaling and/or root planing during pregnancy” Polyzos et al. Am J Obstet Gynecol. 2009 Mar;200(3):225-32.