CEREBELLUM
Chapter 15. CEREBELLUM. Dr. Mohammed Alanazy. Outline. Localization of cerebellar lesions Cerebellar lobes, peduncles, and deep nuclei Microscopic circuitry of the cerebellum Cerebellar output pathways Cerebellar input pathways Vascular supply to the cerebellum Cases.

CEREBELLUM
E N D
Presentation Transcript
Chapter 15 CEREBELLUM Dr. Mohammed Alanazy
Outline • Localization of cerebellar lesions • Cerebellar lobes, peduncles, and deep nuclei • Microscopic circuitry of the cerebellum • Cerebellar output pathways • Cerebellar input pathways • Vascular supply to the cerebellum • Cases
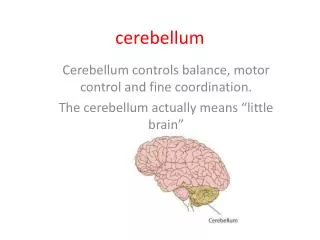
The cerebellum integrates massive sensory and other inputs from many regions of the brain and spinal cord, and uses these inputs to smoothly coordinate ongoing movements and to participate in motor planning.
Localization of cerebellar lesions: • Ataxia is ipsilateral to the side of a cerebellar lesion. • Midline lesions of the cerebellar vermis or flocculonodular lobes mainly cause unsteady gait ( truncal ataxia) and eye movements abnormalities, which are often accompanied by intense vertigo, nausea, and vomiting. • Lesions lateral to the cerebellar vermis mainly cause ataxia of the limbs ( appendicular ataxia).
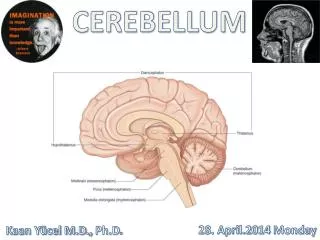
Cerebellar lobes, peduncles, and deep nuclei • The cerebellum consists of a midline vermis, and two large cerebellar hemispheres. • Fissures: • The primary fissure ( separates ant. and post lobes) • The posterolateral fissure ( separates posterior lobe from flocculonodular lobe) • The two flocculi are connected to the midline structure called the nodulus. • The nodulus is the most inferior portion of the cerebellar vermis. • Cerebellar tonsils: on the inferior portion of the cerebellum ( crucial to know about tonsillar herniation)
Cerebellar peduncles form the walls of the forth ventricle. • Superior cerebellar peduncle = brachium conjunctivum • Middle cerebellar peduncle = brachium pontis • Inferior cerebellar peduncle = resiform body (ropelike body).
The superior cerebellar peduncle carries mainly outputs from the cerebellum. • The superior cerebellar peduncles decussate in the midbrain at the level of the inferior colliculi. • The middle and inferior carry mainly inputs.
The cerebellum can be divided into three functional regions, from medial to lateral, based on their input and output connections:
The deep cerebellar nuclei and vestibular nuclei also fit with this medial to lateral functional organization. • All outputs from the cerebellum are relayed by these nuclei. • In addition, these nuclei receive collateral fibers of cerebellar inputs on their way to the cerebellar cortex.
The deep cerebellar nuclei are (from lateral to medial): • Dentate • Emboliform • Globose • Fastigial ( Don’t Eat Greasy Food)
The dentate receives projections from the lateral cerebellar hemispheres • The emboliform and globose (interposed nuclei): inputs from the intermediate part of the cerebellar hemispheres. • The fastigial: inputs from the vermis, and a small inputs from the flocculonodular lobe. • Most fibers leaving the inferior vermis and flocculi project to the vestibular nuclei, which function in some ways like additional deep cerebellar nuclei.
Microscopic circuitry of the cerebellum • Layers of Cerebellar cortex • Synaptic inputs • Mossy fibers • Climbing fibers • Inhibitory interneurons in the cerebellar cortex • Basket cells • Stellate cells • Golgi cells
Cerebellar cortex has three layers: • The molecular cell layer • The Purkinje cell layer • The granule cell layer
There are two kinds of synaptic inputs: • Mossy fibers: • Arise from numerous regions • Ascend through cerebellar WM to form excitatory synapses onto dendrites of granule cells • Granule cells send axons into the molecular layer, which bifurcate, forming parallel fibers that run parallel to the folia. • The parallel fibers run perpendicular to the dendrites of the Purkinje cells. • Each parallel fiber forms excitatory synaptic contacts with numerous Purkinje cells. • All output from the cerebellar cortex is carried by the axons of Purkinje cells into the cerebellar wm. • The Purkinje cells form inhibitory synapses onto the deep cerebellar nuclei and vestibular nuclei, which then convey outputs from the cerebellum to other regions through excitatory synapses.
Climbing fibers: • Arise exclusively from neurons in the contralateral inferior olivary nucleus. • They wrap around the cell body and proximal dendritic tree of Purkinje cells, forming powerful excitatory synapses. • Climbing-fiber inputs have a strong modulatory effect on the response of the Purkinje cells, causing a sustained decrease in their response to synaptic inputs from parallel fibers.
Inhibitory interneurons in the cerebellar cortex • Basket cells • Stellate cells • Golgi cells
All axons projecting upward are excitatory. All axons projecting downward are inhibitory.
Cerebellar output pathways • Lesions of the lateral cerebellum distal limb coordination • Medial lesions affect mainly trunk control, posture, balance, and gait. • Deficits occur ipsilateral to the lesion (why?) • Output pathways from the cerebellum are double crossed ! • In superior cerebellar peduncle • In corticospinal and rubrospinal tracts. • Each cerebellar hemisphere receives information about the ipsilateral limbs.
Output from the cerebellum are carried by Purkinje cells to the deep cerebellar nuclei or vestibular nuclei. • Output from the lateral cerebellar hemisphere • Via Dentate nucleus ( motor planning) • Output from the intermediate cerebellar hemisphere • Via interposed nuclei (influencing laterl motor systems) • Output from the cerebellar vermis and flocculonodular lobe hemisphere • Via fastigial nucleus ( influencing medial motor system) • The flocculonodular lobe and inferior vermis also have direct projections to the vestibular nuclei influencing balance and vestibulo-ocular control.
Output from the lateral cerebellar hemisphere There is some evidence that output from the lateral cerebellum relay in the thalamus to reach the prefrontal association cortex, possibly playing a role in cognitive function Motor, premotor, supplementary motor area Parietal lobe influence motor planning in the corticospinal system.
Output from the cerebellar vermis and flocculonodular lobe hemisphere Influence anterior corticospinal tract Vestibulo-ocular reflexes and Smooth pursuit III CN MLF VI CN Tecto-spinal Equilibrium and balance
The Vestibulo-Ocular Reflexes • Because of inertia, rotation of the head in a counterclockwise direction causes endolymph to move clockwise with respect to the canals. This reflects the stereocilia in the left canal in the excitatory direction, thereby exciting the afferent fibers on this side. In the right canal the hair cells are hyperpolarized and afferent firing there decreases.
Cerebellar input pathways • Inputs to the cerebellum have a rough somatotopic organization, with the ipsilateral body represented in both the anterior and posterior lobes.
1. Corticopontine fibers Frontal, temporal, parietal, occipital cortices Internal capsule Cerebral peduncles cerebellum Middle cerebellar peduncles, mossy fibers Pontine nuclei
Dorsal spinocerebellar ( LE) and Cuneocerebellar tracts(UE): Unconscious information reach the ipsilateral cerebellum provide rapid feedback to the cerebellum about ongoing limb movements, allowing fine adjustments to be made. Ventral spinocerebellar ( LE) and rostral spinocerebellar ( UE) tracts: Information about activity of spinal cord interneurons Arms Legs
3. Inferior olivary nucleus Climbing fibers Inferior cerebellar peduncle
4. Vestibular inputs • Fibers from vestibular ganglia and vestibular nuclei project to the ipsilateral inferior cerebellar vermis and flocculonodular lobe via the juxtarestiform body.
Inferior cerebellar peduncle: consists of two divisions: • Restiform body is an afferent fiber system containing: (1) Dorsal spinocerebellar tract (2) Cuneocerebellar tract (3) Olivocerebellar tract • Juxtarestiform body contains afferent and efferent fibers: (1) Vestibulocerebellar fibers (afferent) (2) Cerebellovestibular fibers (efferent) Middle cerebellar peduncle connects the cerebellum to the pons • pontocerebellar fibers to the neocerebellum. Superior cerebellar peduncle connects the cerebellum to the pons and midbrain. represents the major output from the cerebellum. • Efferent pathways (1) Dentatorubrothalamic tract (2) Interpositorubrothalamic tract (3) Fastigiothalamic tract (4) Fastigiovestibular tract • Afferent pathways (1) Ventral spinocerebellar tract (2) Trigeminocerebellar fibers (3) Ceruleocerebellar fibers
Lateral medulla, • most of the inferior half of the cerebellum, • the inferior vermis • Inferior lateral pons, • MCP, and • a strip of anterior cerebellum • Flocculus • Upper lateral pons, • SCP, • most of the superior half of the cerebellum, • deep cerebellar nuclei and • superior vermis
Clinical pearls • Infarcts are more common in PICA and SCA • Often, lateral medulla and pons are involved: • Look for brainstem signs and symptoms • Infarct that spare lateral brainstem and involve mainly cerebellum are more common with SCA. • Large infarct can cause swelling of the cerebellum hydrocephalus or brainstem compression and tonsilar herniation.( monitor pt closely for at least 72 hours) • Same with cerebellr hemorrhage
If you see a patient with • Wide-based, unsteady “drunklike gait” • Truncal ataxia • Lesion in cerebellar vermis • Ataxia on movement of the limbs only • Appendicular ataxia • Lesion in ipsilateral cerebellar hemisphere sparing the vermis • Both of the above • Lesion in the cerebellar hemisphere extending to the vermis
False localization of ataxia • Lesion of the cerebellar peduncles or pons can produce severe ataxia without involvement of cerebellar hemispheres • Can produce gait abnormalities resemble cerebellar truncal ataxia: • Hydrpcephalus ( may damage frontopontine pathways • Lesions of the prefrontal cortex • Spinal cord lesions • Ataxic hemiparesis • Lesion in corona radiate, internal capsule, or pons, disrupting corticospinal and corticopontine fibers • Sensory ataxia