Occult Rectal Prolapse
Occult Rectal Prolapse. M62 Course 2007 David Jayne St. James's University Hospital, Leeds. Occult Rectal Prolapse. Internal rectal prolapse Rectal intussusception Full-thickness invagination of the distal rectum during the act of defaecation. Occult Rectal Prolapse. Asymptomatic

Occult Rectal Prolapse
E N D
Presentation Transcript
Occult Rectal Prolapse M62 Course 2007 David Jayne St. James's University Hospital, Leeds
Occult Rectal Prolapse • Internal rectal prolapse • Rectal intussusception • Full-thickness invagination of the distal rectum during the act of defaecation
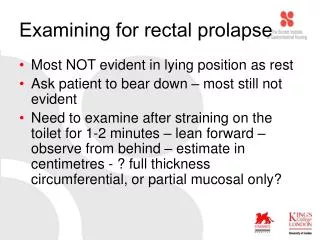
Occult Rectal Prolapse • Asymptomatic • 50 – 60% proctograms in normal volunteers • Symptomatic • Solitary Rectal Ulcer Syndrome • Obstructed Defaecation Syndrome (ODS) • Faecal incontinence
Obstructed Defaecation Syndrome (ODS) • Under-diagnosed • 15 – 20% women • More common in multiparous • Symptoms • Straining • Laxative / Enema dependency • Incomplete evacuation • Fragmented defaecation • Rectal pain • Perineal support / Digitation
Occult Rectal Prolapse • Central to the concept of ODS • Co-existent • Rectocele • Muco-haemorrhoidal prolapse • Enterocele / Sigmoidocele • Descending perineum • Urogenital prolapse
A unifying theory for ODS • Chronic straining produces a stretching and redundancy of the distal (subperitoneal) rectum • Rectal redundancy is the anatomical defect underlying ODS
Rectal Redundancy • Internal prolapse – rectal invagination • Rectocele – transverse distension • Perineal descent – distal elongation • Initial compensatory mechanisms • Facilitate opening of the rectal lumen • Gradual impaired ability to generate intra-rectal pressure for evacuation
Rectal Redundancy • Dependency on extra-rectal forces to achieve rectal evacuation • Enterocele / Sigmoidocele • Descending perineum • May be dynamic or become stable
Concept • Correction of ODS requires excision of the redundant rectum and its associated structural abnormalities
STARR ProcedureStapled Transanal Rectal Resection • Aims to correct the anatomical defects associated with ODS by resection of the redundant distal rectum • Previously double stapling technique using x2 PPH-01 guns • New Transtar method
33mm stapler Curved Cutter Reloadable staple cartridge Transtar stapler
CAD inserted & secured Transtar procedure
Leading edge of prolapse identified Transtar procedure
4x gathering sutures 2, 10, 8 & 4 o’clock Traction 5th suture to aid first “radial cut” Transtar procedure
Radial cut Determines “height” of specimen Direct vision Traction of 2 & 4 o’clock gathering sutures Transtar procedure
2nd firing Circumferential resection Direct vision Tension on 2 & 10 o’clock gathering sutures Transtar procedure
Circumferential resection Direct vision “Sausage” specimen Transtar procedure
Complete circumferential resection Beginning & end points meet up Prolapse excised Transtar procedure
Full-thickness circumferential resection of distal rectum Transtar procedure
Summary • Internal rectal prolapse, rectocele & muco-haemorrhoidal prolapse all manifestations of posterior pelvic floor dysfunction • Primary defect is redundancy of the distal rectum • Correction of rectal redundancy addresses the anatomical defect and is advocated for the treatment of ODS
Internal Rectal Prolapse M62 Course 2007 David Jayne St. James's University Hospital, Leeds
Internal Rectal Prolapse M62 Course 2007 David Jayne St. James's University Hospital, Leeds
Internal Rectal Prolapse Distal Rectal Redundancy M62 Course 2007 David Jayne St. James's University Hospital, Leeds