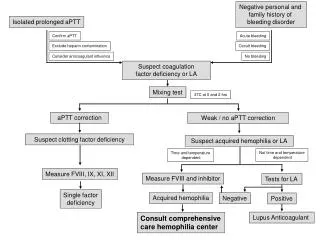
APTT
APTT. Causes of prolonged aPTTs: 1. Spurious (common to many Coag tests) : dilution (saline, Tx), underfilled specimen, clotted, prolonged tourniquet time Heparin (therapeutic, SC, lines (esp ICU, dialysis), wrong tube for collection)

APTT
E N D
Presentation Transcript
Causes of prolonged aPTTs: 1. Spurious (common to many Coag tests): • dilution (saline, Tx), underfilled specimen, clotted, prolonged tourniquet time • Heparin (therapeutic, SC, lines (esp ICU, dialysis), wrong tube for collection) • Polycythemia (Hct >45 causes citrate ratio to be incorrect) • Presence of an inhibitor. • lupus anticoagulant (LAC) - very common esp with Platelin LS reagent as LAC sensitive • VIII or other acquired inhibitor (rare except in Haemophilia centre or elderly patient) 3. Factor deficiency: • Congenital deficiency of 1/more intrinsic clotting factors or vWF (not FVII). • Severe Vitamin K deficiency (II, IX ,X) or warfarin overanticoagulation • Liver disease (also reduces AT3, Prot C/S) • includes dys/hypofibrinogenaemia 4. DIC (FDP effect and factor consumption, including fibrinogen) 5. 2.5% “normal population” have APTT > NR (by definition) • Excess LMWH or danaparoid (Xa activity >> IIa effect), hirudins Causes of shortenedAPTTs: • activated specimen/started to clot (esp NICU samples, check for clots, rebleed) • FVIII (acute phase reactant) • delayed analysis UFH Tx patient specimen after collection (release of PF4 neutralises heparin) • 2.5% pop have APTT <NR (by definition)
Coagulation Factor Plasma Concentration Plasma T1/2 Life Fibrinogen 2500-3500 mg/ml 80-90 hrs Prothrombin 100-150 mg/ml 60-70 hrs Factor V 5-10 mg/ml 15-25 hrs Factor VII 0.5 mg/ml 4-7 hrs Factor VIII:C 0.1-0.2 mg/ml 8-16 hrs Factor IX 3 mg/ml 12-24 hrs Factor X 10-15 mg/ml 40-45 hrs Factor XI 2-7 mg/ml 40-84 hrs Factor XII 29-40 mg/ml 40-60 hrs Factor XIII 20 mg/ml 120 hrs Prekallikrein 25-45 mg/ml approx. 35 hrs HMWK 70-90 mg/ml 150-160 hrs
Causes of high PT • liver disease • DIC • congenital deficiency: II, V, VII, X or fibrinogen (rare) • nephrotic syndromes (loss of clotting factors) • presence of an inhibitor (factor or rarely LAC) • poorly collected specimen eg. • over-filled specimen • under-filled specimen • vitamin K deficiency (eg diet/malabsorption) • warfarin • gross over-heparinization Shortened INR’S usually indicate activation of the specimen during collection by skin/traumatic venepuncture
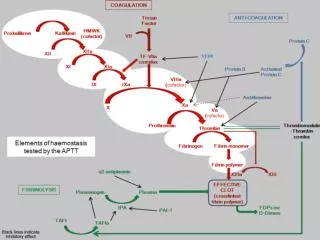
INTRINSIC EXTRINSIC Fibrinogen FDPs TCT Clot Stability Test
fondaparinux pure anti-Xa S S S LMWH mainly <18 saccharide units eg. enoxaparin - Xa:IIa 3.9:1 S S S S S S S S S protamine LMWH et al. vs UFH danaparoid - Xa:IIa 28:1 - not a heparin UFH >18 saccharide units with sulphonated tail- Xa:IIa 1:1