Download
1 / 22
280 likes | 828 Vues
Occipital Headaches (Occipital Neuralgia). Demonstration of a Technique to Unlock the Occipto-atlantal (O-A) joint By Jeffrey Pearson, D.O. www.medicine-in-motion.com. Occipital Headaches. Type of headache that results from restriction/locking of one or both occipito-atlantal (O-A) joints.

E N D
Occipital Headaches(Occipital Neuralgia) Demonstration of a Technique to Unlock the Occipto-atlantal (O-A) joint By Jeffrey Pearson, D.O. www.medicine-in-motion.com
Occipital Headaches • Type of headache that results from restriction/locking of one or both occipito-atlantal (O-A) joints. • These are the two joints on the very top vertebra in the neck (the atlas) • Imagine 2 “cups” on either side of the atlas. The base of the skull (occiput) rests balanced in them.
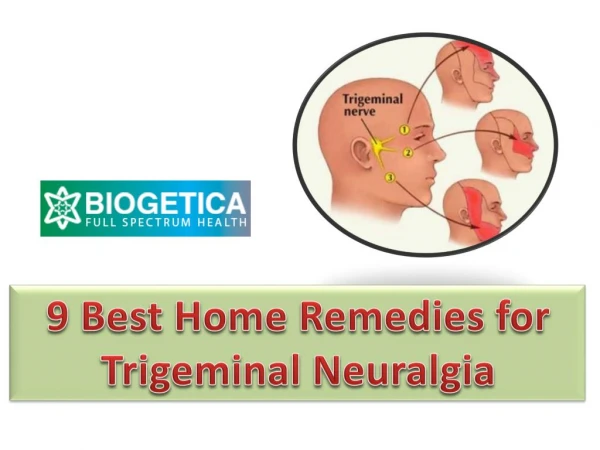
Occipital Headaches • In the vicinity of the O-A joints lie the muscles of the suboccipital triangle and the greater occipital nerve. • This nerve runs from the base of the skull, up and around the skull.
Occipital Headaches • Awkward, static postures can cause one or both O-A joints to lock. • Discomforts often NOT felt at the time. • Symptoms generally develop over course of subsequent hours.
Occipital Headaches • Most commonly present as unilateral (one-sided), throbbing headache often associated with nausea, dizzy/woozy sensations with movement. • Often confused with migraine headaches.
Occipital Headaches • Headaches need not be present to cause symptoms. • May present with sudden dizziness or unexplained nausea • Better term for this condition is occipital neuralgia • Irritation of nerve may induce autonomic nervous system reflex symptoms • E.g. hitting finger with hammer may be associated with nausea in addition to the pain.
Occipital Headaches • Postures commonly associated with occipital neuralgia/headaches: • Tucking telephone under chin • Poor computer ergonomics • Monitor too high/too low • Watching TV while lying on couch • Reading in bed • Working above your head • Trimming trees, painting, etc
Occipital Headaches • May be acute • Atraumatic (e.g. “Honey do’s”) • Paint the ceiling • Prune trees • Fix the plumbing under the sink • Head trauma • Sports and motor vehicular injuries
Occipital Headaches Often chronic Chronic headaches are attributed to a variety of things including withdrawal from caffeine, pain relievers, etc. We are creatures of habit; hence we tend to perform similar tasks using similar postures on a repetitive basis over time. Receptionist using telephone without headset. Kids playing video games on the floor while looking up at television screen.
Occipital Headaches • Treatment • Acute • ICE • Unlock the joint (GENTLE mobilization) • Pain relievers • Naproxen sodium (Aleve), Tylenol, narcotics • Chronic • prevention
Occipital Headaches • Do it yourself treatment options • You must be very gentle! • Any fast attempts will be met with reflex spasm, making mobilization difficult. • Also want to avoid further injury.
Occipital Headaches • 3 planes of motion • Flexion/extension • Extension: gazing up at the ceiling • Flexion: touching chin to chest • Sidebending • Touching ears to shoulders • Rotation • Turning head/neck to look over shoulder
Occipital Headaches • 1. Palpate both O-A joints using index fingers
Occipital Headaches • 2. Extend your neck backwards to gaze up at the ceiling.
Occipital Headaches • 3. Sidebend to one side, then gently rotate your head to the opposite side • It’s as if you were trying to look back and up at a star over your shoulder.
Occipital Headaches • 4. Slowly work your way around towards the other side, monitoring the O-A joints all of the time.
Occipital Headaches • If you’re REALLY gentle, you might be able to feel the restricted joint “unlock.” • Then apply some ice and consider an over-the-counter anti-inflammatory/analgesic agent such as Aleve.
Occipital Headaches • Alternative maneuver • Lie supine (face up) with a towel roll supporting your neck (possibly with a cold gel pack) • Slowly allow your neck to gently rotate from one side to another, back and forth. If you can relax enough, the joint might “unlock.” • Follow-up with Aleve, as before.
Occipital Headaches • Recurrences/chronic headaches • Best treatment is prevention • Look at daily postures both at home and at work. • Fix poor ergonomics. • Use telephone headsets; adjust computer monitors. • Avoid awkward neck postures. [If you cannot, try to apply ice and perform some gentle range-of-motion stretching/exercises as soon as possible to prevent things from locking up.]
Occipital Headaches • If you have symptoms of occipital neuralgia and they do not respond to these simple home maneuvers, contact your physician to verify diagnosis. • If true migraine, should respond to a “triptan” type of medication. • If elderly, stroke might need to be ruled out.
Occipital Headaches • Sometimes, the joint(s) are so restricted that not even a physician/chiropractor can unlock it. • Consider nerve block • Inject local anesthetic (without a steroid) into the affected suboccipital triangle. • Generally lasts 4-6 hours; patient goes home to rest and perform the previously described “alternative maneuver.” The hope is that the anesthetic will permit the local muscles to relax enough to finally unlock. • “Good drugs” • Muscle relaxants, analgesics (“pain killers”) such as Fioricet, hydrocodone. • These might make subsequent attempts, later on in week, at mobilization easier.