Download
1 / 18
180 likes | 294 Vues
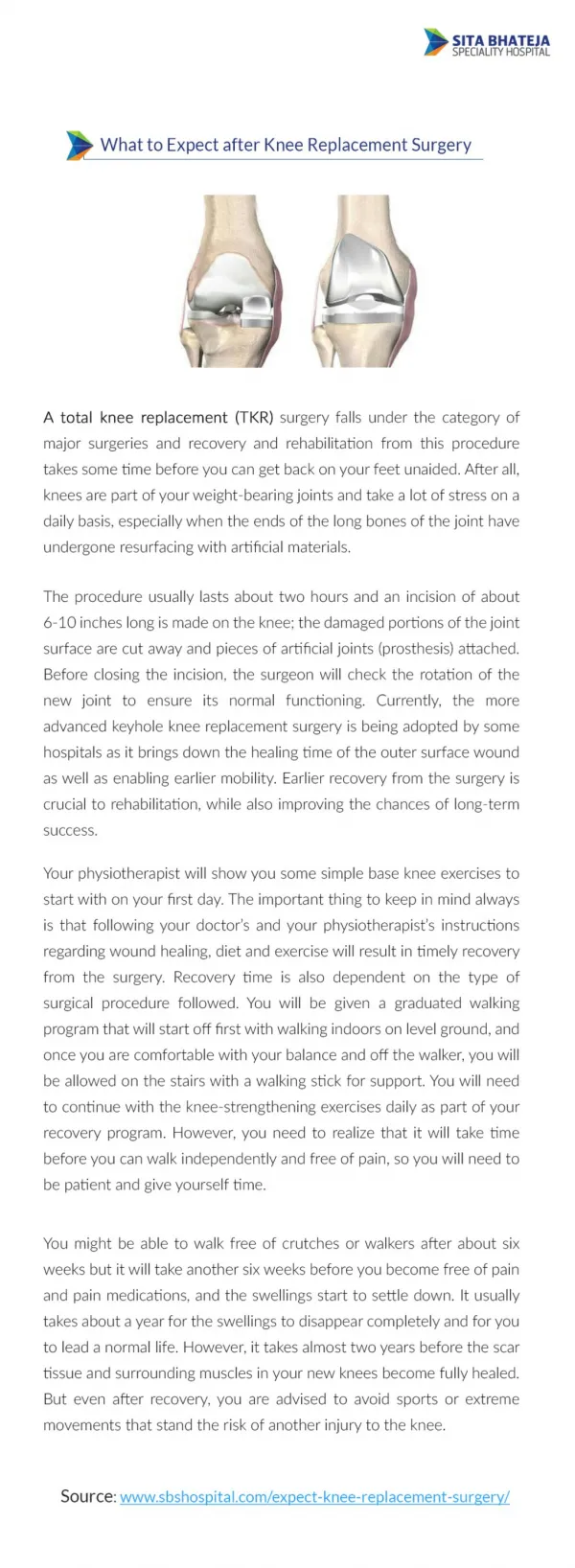
Intraoperative Small-Dose Ketamine Enhances Analgesia After Outpatient Knee Arthroscopy. Elizabeth Mann, RN, BSN, SRNA Oakland University-Beaumont Hospital Graduate Program of Nurse Anesthesia February 8, 2012. Article.

E N D
Intraoperative Small-Dose Ketamine Enhances Analgesia After Outpatient Knee Arthroscopy Elizabeth Mann, RN, BSN, SRNA Oakland University-Beaumont Hospital Graduate Program of Nurse Anesthesia February 8, 2012
Article Menigaux, C., Guignard, B., Fletcher, D., Sessler, D.I., Dupont, X., Chauvin, M. (2001). Intraoperative small-dose ketamine enhances analgesia after outpatient knee arthroscopy. Anesthesia & Analgesia 93, 606-12.
Background • Ketamine had been previously been tested in inpatient arthroscopic anterior ligament repair proving better pain relief and faster return to normal functional activity • Standard treatment for outpatient arthroscopy at the time of study • NSAIDs alone • Combination with intraarticular Bupivacaine and morphine.
Hypothesis • A small intraoperative dose of Ketamine will improve postoperative analgesia and facilitate ambulation after arthroscopic meniscectomy and that the benefits will last for several days.
Study • Double blinded study • 50 patients: 25 in Control Group and 25 in Ketamine Group • Inclusion Criteria: • Patients were all scheduled for elective arthroscopic surgery • ASA status I and II • Between the ages of 18-60
Exclusion Criteria • ASA status >II • Surgery performed under regional anesthesia • History of chronic pain • Chronic use of analgesic medications • Drug or alcohol abuse • Psychiatric disorders • Contraindications to NSAIDs
Pain Assessment Tools • Verbal rating scale (VRS) and visual analog scale (VAS) while ambulating • VAS: 0-100 mm, 0 is no pain and 100 is worst pain • VRS: • 0= no pain • 1= light pain • 2= moderate pain • 3= intense pain • 4= severe pain
Methods • Consent was obtained • The hospital pharmacist prepared a 10 mL syringe of either isotonic sodium chloride or 0.15 mg/kg Ketamine diluted in isotonic sodium chloride • The group assignments were made with a computer generated random number table • Patients and OR Staff were unaware of their group assignment
Methods • Patients were premedicated with 100mg hydroxyzine PO, 1-2 hours before surgery • Induced with Propofol (2mg/kg) followed with Alfentanil (20mcg/kg) • LMA inserted • Mechanically ventilated • GA maintained with Propofol gtt (60-200 mcg/kg/min) • Titrated to maintain HR and MAP within 20% of preoperative vitals • 60% N2O in oxygen
Methods • Same surgeon • Same technique • Every patient received 20 mL 0.5% Bupivacaine and 5 mg of Morphine injected into knee joint before tourniquet deflation • Propofol gtt was discontinued after trocars were removed from the knee
Methods • Transferred to PACU • 3 mg IV Morphine (every 5 minutes/PRN) until VAS score was <30 mm or VRS score was <2 • Patients received 550 mg Naproxen PO • Patients were discharged home • Instructed to take 550 mg Naproxen twice daily • 2 tablets of Di-Antalvic every 6 hours for pain (400 mg Acetaminophen/30 mg dextropropoxyphene) • Resume normal activity as soon as they could
Measurements in PACU • Pain scores were evaluated at both rest and mobilization • Recorded every 15 minutes x 1 hour, then at 2, 4, and 6 hours after surgery • Mobilization assessment stopped • VAS score >30 mm • VRS >2 • Sedation score > 2 (patient somnolent, responds to tactile stimulation) • HOTN (MAP <60) or Bradycardia (HR <50)
Questionnaires POD 1-3 • Assessed pain during the night, at their first step, and an over all rating (VAS) • Number of painful events during the day (0-5, 6-10, >10) • Duration of walking during that day (0, <1 hour,1-3 hour, or normal) • Number of doses of Di-Antalvic and any concomitant medication used during the day • Side effects • Whether they experienced bad dreams • Global score of patient satisfaction with pain control
Data Analysis • Primary end point: Post-op pain • Secondary end point variables: Analgesic consumption and return to normal walking. • Statistical analysis was performed with NCSS 6.0 • Unpaired Student T-tests • Age, weight, length of surgery, amount of Propofol and Alfentanil • Time intervals to SV, LMA removal, arrival to PACU, and discharge home
Data Analysis • Mann-Whitney U-test • Analgesic doses, sedation scores, and pain episodes • X2 • Frequency of side effects • Results presented as +/- SD or median and 25-75th percentile ranges • P< 0.05 was considered statistically significant
Results • Control group required more Morphine titration in PACU (P<0.05) • Ketamine group had lower VAS scores in PACU while ambulating • Pain scores were lower in the Ketamine group (POD 1-3) • During the night • At their first step • During ambulation • Ketamine group required less additional narcotic (POD1-3) • There were no reports of N/V, dysphoria, hallucinations, diplopia, cognitive or memory impairmentsin both groups
Strengths/Limitations • Strengths • No patients were excluded • All 50 patients returned the follow up questionnaire • Double Blind Study • Limitations • Small sample size • Difficult to study pain due to subjective measurements
Conclusion • This study extended previous studies that evaluated small dose ketamine benefits for inpatient orthopedic procedures. • It provided evidence that a balanced technique with Ketamine could provide better analgesia and improve ambulation without increasing adverse effects.