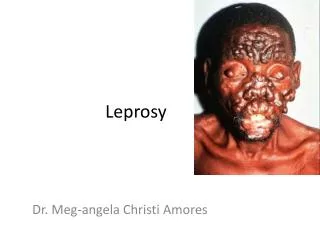
Hansen’s Disease
Hansen’s Disease. History. Definition: Leprosy is a chronic systemic disease caused by Mycobacterium leprae manifesting as development of specific granulomatous or neurotrophic lesions in the skin, mucous membrane, eyes nerves, bones and viscera. Oldest infection known to mankind

Hansen’s Disease
E N D
Presentation Transcript
History • Definition: Leprosy is a chronic systemic disease caused by Mycobacterium lepraemanifesting as development of specific granulomatous or neurotrophic lesions in the skin, mucous membrane, eyes nerves, bones and viscera. • Oldest infection known to mankind • Synonyms: Hansen’s disease, ‘Kushtharoga’
Transmission of Leprosy • Respiratory route: inhalation of bacilli-laden droplets • Cutaneous: skin to skin contact • GIT : ingestion of food • Intradermal : inoculation by tattoos } Not Yet Proven
Epidemiological factors • Occurs at all age groups • Peak age of onset : Between 10 – 20 years • Males > Females • Children most susceptible • Immune status ( host resistance) • Overcrowding • Low socioeconomic status
Immunity and Leprosy Clinical manifestation No infection Subclinical infection with spontaneous regression Indeterminate, pure neuritic, tuberculoid Mid-borderline, borderline-lepromatous Lepromatous Host resistance • Excellent • Good • Fair • Poor • Very poor
Mycobacterium Leprae • Obligate, intracellular, acid-fast bacillus • Affinity for skin, nerves and muscle tissue • Found in macrophages, histiocytes and Schwann cells. • Non cultivable • Grown in animal models • Closely resembles M.tuberculosis, but less acid-fast. • Multiplies in 11-13 days.
Classification The Ridley Jopling classification • Indeterminate • Tuberculoid • Borderline: borderline-tuberculoid, mid-borderline, borderline-lepromatous • Lepromatous Pure neural, Maculoanaesthetic - Indian classification
Classification • Paucibacillary Leprosy(PB): Indeterminate leprosy (I) Tuberculoid leprosy (TT) Borderline tuberculoid (BT) Pure neuritic (PN)* • Multibacillary Leprosy(MB): Midborderline leprosy (BB) Borderline lepromatous (BL) Lepromatous leprosy (LL) * Asymmetric nerve involvement with no skin lesion and usually of tuberculoid origin.
Tuberculoid (TT) • Single or few, asymmetrical, well-defined, erythematous or copper-coloured patches • Sensations - Absent • Nerves - thickened, presence of feeding nerves, abscesses • Skin smears - Negative • Lepromin test - Strongly positive • Course - Relative benign and stable, with good prognosis.
Borderline leprosy Common type of leprosy • Subdivided into BT, BB & BL. • Course - Unstable with variable prognosis , may progress to sub-polar LL leprosy. • Most prone to reactions. • Lepromin test -Negative ,weakly positive in BT.
Borderline Tuberculoid (BT) • Few asymmetric, hypopigmented or skin colouredmacules, plaques with ill defined margins • Presence of satellite lesion near the advancing margin of patch • Sensory impairment - Marked • Nerve involvement - Marked and asymmetrical
Midborderline leprosy (BB) • Unstable form, reactions frequent • Annular lesions with characteristic punched out appearance (inverted saucer shaped) • Sensory impairment - Moderate. • Nerve involvement - Marked and asymmetrical.
Borderline lepromatous leprosy (BL) • Multiple shiny macules, papules, nodules and plaques with sloping edges • Sensory impairment - Slight • Nerve involvement - Widespread and less asymmetrical. • Glove & stocking hypoaesthesia
Lepromatous leprosy • Hypopigmented, erythematous or coppery, shiny macules, papules, nodules • Lesions symmetrically distributed, small, multiple, shiny with normal or mild sensory loss • Leonine facies: Infiltration of skin with nodules, loss of eyebrows and eyelashes • Nerve involvement symmetrical; glove & stocking anaesthesia • Lepromin test - Negative
Indeterminate leprosy • Asymmetrical, single /multiple hypopigmented, or faintly erythematous and ill-defined macules. • Sensation - Normal or slightly impaired • Peripheral nerves - Normal • Skin smears - Negative • Lepromin test - Unpredictable and variable • Course - Usually self limiting ,may progress to other forms of leprosy.
Pure Neuritic leprosy • Neuritic manifestations -Tingling, heaviness and numbness, paresis, hypotonia, atrophy, claw hand and toes, wrist-drop, foot-drop. No skin lesion. • Other changes-Anhidrotic, dry glossy skin, blisters, neuropathic ulcers, decalcification, bone resorption.
Pure Neuritic leprosy • Lepromin test -Slightly positive. • Course-Spontaneous regression or progression to TT leprosy. • Silent neuritis (silent neuropathy) Sensory or motor impairment without skin signs of reversal reaction or ENL ,tenderness, paraesthesiae or numbness.
Special forms of Leprosy • Lucio Leprosy: Rare form of lepromatous leprosy, described in Mexico. Diffuse widespread infiltration of skin, loss of body hair, loss of eyebrows & eyelashes, and widespread sensory loss. • ‘Lepra Bonita’ (Pretty leprosy) Elderly persons with diffuse infiltration of face smoothes out wrinkles, giving youthful appearance. • Histoid leprosy: BL patients with irregular or poor treatment compliance Drug resistant cases
Eye Involvement in Leprosy • Lagophthalmos (partial/complete, unilateral/bilateral) • Conjunctivitis • Exposure keratitis and corneal ulcers • Madarosis, trichiasis leading to corneal vascularity and opacity • Dacryocystitis (acute,subacute or chronic) • Nodules on sclera, episcleritis, scleritis • Corneal nodules and lepromatous pearls • Microlepromata, nodules on iris and ciliary body
Nerve Involvement in Leprosy • Sensory involvement - Anaesthesia in hands & feet, glove and stocking anaesthesia, repeated trauma • Motor involvement- Wasting and paralysis of muscles • Autonomic involvement -Icthyosis, loss of hair and sweating.
Other features • Nasal stuffiness / crusting • Epistaxis • Hoarseness of voice • Gynaecomastia • Saddle nose • Bone resorption • Lymphadenopathy
Differential diagnosis of leprosy Macular lesions • Vitiligo • Occupational leucoderma • Tineaversicolor • Pityriasis alba • Post kalaazar dermal leishmaniasis • Naevusdepigmentosus • Scars
Differential diagnosis of leprosy Infiltrated lesions • Lupus vulgaris • Lupus erythematosus • Granulomaannulare • Annular syphilides • Post kalaazar dermal leismaniasis (infiltrated lesions) • Sarcoidosis • Psoriasis
Differential diagnosis of leprosy Nodular lesions • Post kalaazar dermal leismaniasis • Cutaneousleismaniasis • Syphilis • Onchocerciasis • Sarcoidosis • Leukaemia cutis • Mycosis Fungoides • Nodules of neruofibromatosis
Differential diagnosis of neurological conditions Sensory impairment with or without muscle wasting • Peripheral neuropathy • Diabetic neuropathy • Primary amyloidosis of peripheral nerves • Congential sensory neuropathy • Syringomyelia • Tabesdorsalis • Thoracic outlet syndrome • Alcoholic neuropathy
Diagnosis Cardinal signs of leprosy • Sensory impairment in affected areas • Enlargement of peripheral nerves associated with signs of peripheral nerve damage • Finding acid-fast bacilli in the lesions
Clinical examination • Type and number of skin lesions • Sensory impairment • Motor examination • Nerve examination • Sweating • Loss of hair
Clinical examination: Sensory • Touch Tested with wisp of cotton,nylon thread or feather. • Temperature Tested with two test tubes – one containing hot water and other cold • Pain Tested by pin prick
Clinical examination : Motor • Testing of motor power- Done clinically • Electro-diagnosis - Employed in very early cases. Electrical stimulator using faradic and galvanic current used to test muscle power.
Nerves • Ulnar • Median • Lateral popliteal • Posterior tibial • Anterior tibial • Sural • Supra/ infraorbital • Greater auricular • Clavicular • Radial • Sup. Radial cut
Investigations for M. Leprae Bacteriological examination Skin smears: Made by slit and scrape method from the most active looking edge of skin lesion and stained with Ziehl-Neelsen method. Reading of smears: Bacteriological index- Indicates density of leprosy bacilli (live & dead) in the smears and ranges from 0 to 6+ Morphological index- It is the percentage of presumably living bacilli in relation to total number of bacilli in the smear
Investigations • Histopathological examination • Nerve biopsy • Sweat function test • Lepromin test • Animal Models: Armadillo, Thymectomised, irradiated nude mice, Korean chipmunk etc.
Newer Investigations • Serological assays: FLA-ABS, RIA, ELISA • PGL, PCR • Other techniques: Chemical, Immunological, Molecular biological, Bioluminescent techniques, Strain specific probes Indications: - To confirm diagnosis in c/o inconclusive histopathological/smear reports. - To distinguish between reaction and relapse - To demonstrate M. leprae or its components - To elicit strain differentiation for molecular epidemiology - To detect drug susceptibility or resistance
MDT-WHO • Paucibacillary leprosy (6 months) - Cap. Rifampicin (600 mg) monthly, supervised - Tab. Dapsone (100 mg) daily • Multibacillary leprosy (1 year) - Cap. Rifampicin (600mg) monthly, supervised - Cap. Clofazimine (300mg) monthly, supervised - Tab. Dapsone (100mg) daily - Cap. Clofazimine (50mg) daily
Blister packets for MDT • Easy to use, handy and of convenient size • Provide complete treatment • Improve clinical attendance • Drugs are better protected against moisture,heat and accidental damage • Ensures quicker dispensing of the drugs • Can be dispensed by non medical person
Other Regimens • ROM Comprises Rifampicin - 600 mgs, Ofloxacin - 400 mgs, Minocycline - 100mg Single dose – single patch (WHO accepted) ROM -6 (Monthly for 6 months) - Paucibacillary ROM -12 (Monthly for 12 months) – Multibacillary
Newer Drugs / Regimens • RO - 28 • Fluoroquinlones - Nalidixic acid • Macrolides (Clarithromycin) • Ansamycin-Rifabutin, Rifapentine • Dihydrofolatereductase inhibitors-Brodimoprim, K-130 • Fusidic acid • Beta-lactam antibiotics • Cephalosporins • Quinolones (Pefloxacin and Sparfloxacin
Immunomodulatory Drugs • Drugs- Levamisole, Zinc • Antigenically related mycobacteria- B.C.G vaccine, M.leprae +B.C.G vaccine, Mycobacterium welchii vaccine, ICRC vaccine. • Other immunomodulators-Gamma interferons,interleukin
Lepra Reactions • Acute episodes or bouts of exacerbations occurring in course of chronic disease • Sudden increase in activity of existing lesions, appearance of fresh lesions with or without constitutional symptoms • Type I reaction - all borderline cases (BT, BB,BL) • Type II reaction - BL & LL cases
Precipitating factors • Physiological conditions like pregnancy • Drugs: anti-leprosy drugs, iodides • Severe physical or mental stress • Infections
Type I Reaction • Sub-types - Upgrading (Reversal) - Downgrading • Type IV hypersensitivity reaction. • Existing lesions worsen/New lesions may appear • Neuritis / Nerve abscesses • Systemic disturbances: Unusual
Type I reaction - complications • Neuritis • Dactylitis, edema of hands & feet, inflammation of small joints of fingers • Corneal anesthesia, Conjunctivitis • Sudden occurrence of claw hand, foot-drop, facial palsy
Type II Reaction • Occurs in BL and LL cases • Type III hypersensitivity reaction • ErythemaNodosumLeprosum-crops of painful, recurrent, erythematous, papulonodular lesions. • Fever and malaise • Iridocyclitis, episcleritis, epididymo-orchitis, arthritis, neuritis, lymphadenitis
Type II Reaction - complications • Frozen hand • Laryngitis • Non-paralytic deformity • Polyarthritis/ RA-like syndrome • Multiple dactylitis • Leucocytosis, Anaemia, raised ESR • Albuminuria/ nephrotic syndrome • Liver/spleen enlargement • Epididimytis/ orchitis, Testicular atrophy/sterility • Gynaecomastia • Adrenal gland hypofunction • Eye involvement
Treatment of Lepra reactions Principles of treatment • Early initiation of treatment for reaction • Continuation / initiation of MDT • Removal of precipitating factor • Rest, physical and mental
Treatment modalities • Analgesics • Corticosteroids • Antimalarials • Clofazimine • Thalidomide • Miscellaneous – colchicine, zinc, cetrizine, antimonials • Supportive management – for eye complications, splints etc.
Deformities in leprosy • Primary: Are caused by the tissue reaction to infection with M.Lepra e.g. leonine facies, flat-nose, claw hand. • Secondary: Occur as a result of damage to the anesthetic parts of the body e.g. planter ulcers, corneal ulcers.
Grading of Deformities/Disabilities: WHO Classification • Grade 0 No anaesthesia, no visible deformity or damage in hands and feet, or no problems in eye or no visual loss • Grade 1 Anaesthesia present, but no visible deformity or damage, eye problems present but vision 6/60 or better. • Grade 2 Visible deformity or damage present in hands or feet , and vision worse than 6/60
Primary deformities • Leonine Facies • Loss of eyebrows and eyelashes • Depressed nose • Gynaecomastia • Palatal Perforation
Secondary deformities • Corneal ulcers and opacities • Plantar ulcers • Palmar ulcers and ulcers on tips of fingers • Resorption • Charcot joints