Download
1 / 99
990 likes | 1.16k Vues
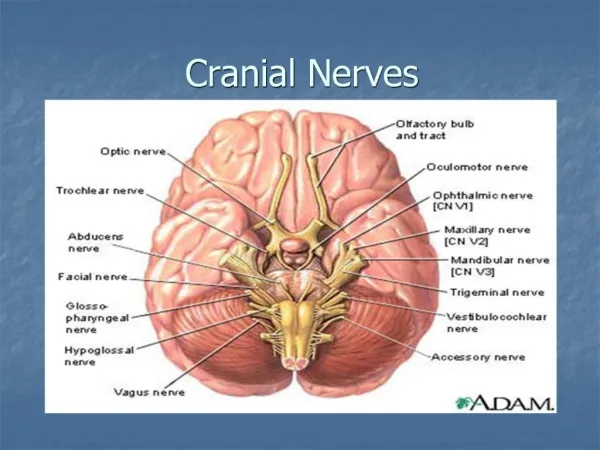
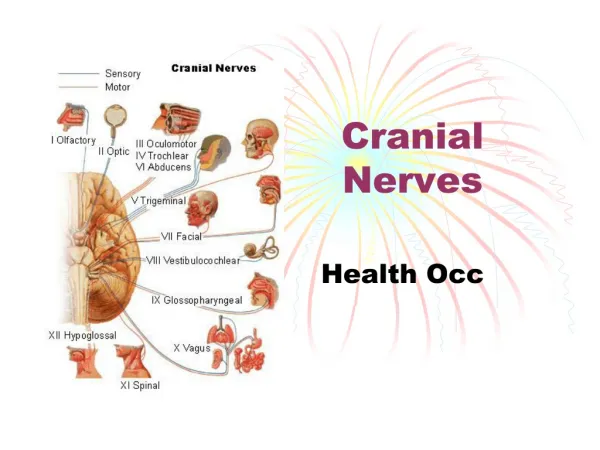
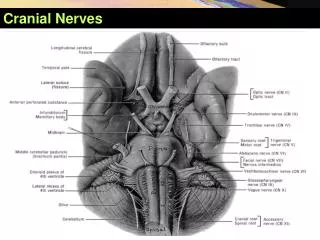
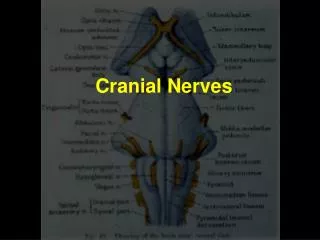
Cranial nerves Dr Massud Wasel MD DO ND BSc (Hons) PGCAP Fellow of Higher Education Academy. Cranial nerve I: olfactory. Applied anatomy. Sensory: smell Motor: none Fibres arise in the mucouse membrane of the nose Axons pass the cribiform plate to the olfactory bulb

E N D
Cranial nerves Dr Massud Wasel MD DO ND BSc (Hons) PGCAP Fellow of Higher Education Academy
Applied anatomy • Sensory: smell • Motor: none • Fibres arise in the mucouse membrane of the nose • Axons pass the cribiform plate to the olfactory bulb • Olfactory tract runs backwards below the frontal lobe and projects, mainly in the uncus of the ipsilateral temporal lobe
Note: olfactory epithelium also contains free ending of 1st division of cranial nerve V
Examination • If the patient complains of anosmia • casual: take a nearby odorous objects like coffee or chocolate and ask the patient if it smells normal • Formal: a series of identical bottles containing smells are used • Coffee, vanilla, comphor, vinegar • Test each nostril separately and determine if any loss of smell is uni-or bilateral.
Findings: Bilateral anosmia: usually nasal, not neurological Causes include URTI, trauma, smoking, old age, Parkinson’s disease. Less commonly, tumours of the ethmoid bones Unilateral anosmia: mucous-blocked nostril, head trauma, subfrontal meningioma
Applied anatomy • The optic nerve begins at the retina • The nerve passes through the optic foramen and joints its fellow nerve from the other eye at the ‘optic chiasm’ • Here the fibres from the nasal half of the retina cross over • They continue in the optic tract to the lateral geniculate body • From there they splay out such that those from the upper retina pass through the parietal lobe and the others through the temporal lobe
The nasal half of the retinal receive input from the temporal part of the visual field in each eye, • The temporal half of the retinal receive input from the nasal half of the eye • Fibres from the nasal halves of the retinas cross, so for example, the left side of the brain receives input from the right side of vision (the left temporal retina and the right nasal retina) and vice versa
Visual acuity • Snellen Chart • Good light, patient stands 6m away • Each eye is tested in turn • Patient reads • Recording • If the patient can’t see any of the letters, record if he/she can: • Count Fingers held in front of his/her face (CF) • See Hand movements (wave your hand) (HM)
Perceive Light (PL) • Record as CF, HM, PL, or NPL (not perceive light)
Visual fields • The area that each eye can see without moving can be mapped out • They are not circular-eyebrows and nose obstruct superiorly and nasally whereas there in no obstruction laterally • Sitting opposite the patient, the examiner’s left visual field (for example) should be an exact mirror image of the patient’s right visual field • In this way the patient’s field can be tested against the examiner’s
Set opposite the patient~1m apart, eyes level • Test first for gross defects and visual neglect with both eyes open • Raise your arms up and out to the sides so that one hand is in the upper right quadrant of your vision and one in the upper left • Ask the patient to look directly at you • Move one index finger and ask the patient to point the hand which is moving • Test with the right, left and then both hands
Test the lower quadrant in the same way • If visual neglect is present the patient will be able to see each hand moving individually but reports seeing only one hand when both are moving
Testing each eye • In the same position as above ask the patient to cover his right eye while you cover your left • If you were now to trace the outer borders of your vision in the air half way between yourself and the patient, if should be almost identical to the area seen by the patient
Test each quadrant individually • Stretch your arm out and up so that your hand is just outside your field of vision, and equal distance between you and the patient • Slowly bring your hand into the centre (wiggling one finger)and ask to say ‘yes’ as soon as he can see it • You should both be able to see your hand at the same time • Test upper right and left , lower right and left individually, bringing your hand in from each corner of vision at a time
Map out any areas of visual loss in details , finding borders. Test if any visual lossextends across the midline horizontally or vertically • Test each eye in turn • Repeat the above procedure with a red-headed pin or similar small red object to map out areas of visual loss in more details • Ask the patient to say ‘yes’ when he sees the pin as red
Start by mapping out the blind spot which should~15 degrees lateral from the centre at the midline • Decide if any defect is of a quadrant, half the visual field or another shape and in which eye, or both • Record by drawing the defect in 2 circles representing the patient’s visual fields
Common visual fields defects • Tunnel vision: • A constricted field, giving the impression of looking down a pipe or tunnel may be caused by glaucoma, retinal damage or papilloedema
Enlarged blind spot; • Caused by papilloedema
acute anterior optic neuritis (papillitis),swelling of the optic disc, unassociated with peripapillary hemorrhages • Unilateral field loss: • Blindness in one eye caused by devastating damage to the eye, its blood supply or optic nerve
Central scotoma: • A hole in the visual field (macular degeneration, vascular lesion) • If bilateral may indicate a very small defect in the corresponding area of the occipital cortex (MS)
Bilateral hemianopia: • The nasal half of both retinas and therefore the temporal half of each visual field is lost (damage to the centre of the optic chiasm such as pituitary tumour, craniopharyngioma, suprasellar meningioma)
Binasal hemianopia: • The nasal half of each visual field is lost (very rare)
Homonymous hemianopia; May be left or right Commonly seen in stroke patients The right or left side of vision in both eyes is lost (e.g. the nasal in the right and the temporal field in the left eye)
Homonymous quadrantanopia: Corresponding quarters of the vision is lost in each eye (e.g. the upper temporal field in the right and the upper nasal field in the left) Upper quadrantanopias suggest a lesion in the temporal lobe Lower quadrantanopias suggest a lesion in the parietal lobe
Ophtalmoscopy • Needs practice • Examination of fundus—difficult • Can view fundus, macular region and retinal vascular arcades • For a complete ophtalmoscopy it is often worth dilating the pupil by mydriatic (1% tropicamide or cyclopentolate)
Dark room • Ask the patient to focus on a distant object • Look through the ophtalmoscope~30 cm away from the patient and bring the light in nasally from the temporal field to land on the pupil • The pupil will appear red and opacities in the visual axis will appear as black dots or lines • By cycling through the different lenses of the ophtalmoscope you should be able to gain an impression of where these opacities lie
Possible locations are the cornea, aqueous, lens (and its anterior and posterior capsules) and vitreous • Dial up a hypermetropic (plus) lens on the ophtalmoscope to focus on the corneal surface and move in as close as possible to the patient’s eye-by gradually decreasing the power of the lens you can examine the cornea, iris and lens in turn • Continue to decrease the power of the lensuntil you can sharply focus on the retinal vessels
It is often best to pick up one of the vascular arcades in the periphery and track them in towards the optic disc • This allows the peripheral quadrants to be examined in turn before viewing the optic disc • Take time to look at the vessels carefully, particularly where the arteries cross the veins • Ask the patient to look directly into the light of the ophtalmoscope to gain a view of the macular region
The normal fundus The optic disc • The healthy disc is a pale pink/yellow colour and round or slightly oval in shape. • The margins between the disc and the surrounding retina should be crisp and well defined. Occasionally a surrounding ring is present which may be slightly lighter or darker in colour. • At the centre of the disc is the physiological cup. It appears paler in colour compared to the rest of the disc.
The macular region • Located temporally from the optic disc • This is the region with the maximum concentration of cones. • At the centre of the macula is the fovea- a tiny pit devoid of blood vessels and responsible for fine resolution. • Disease involving the macula and fovea can cause devastating visual loss.
The retinal vessels • The central retinal artery and vein enter and leave the globe in the centre of the optic disc. • Veins appear larger and darker in colour in comparison to the arteries. • Spontaneous venous pulsations are seen in many normal eyes. • Arterial pulsations should not be visible in normal eyes.
Abnormal findings on fundoscopy Optic disc swelling Appearance • The optic disc is raised, swollen, and enlarged. • The disc often appears darker in colour. • The margins of the disc are blurred and become indistinct from the adjacent retina. • Retinal vessels can be seen arching down from the disc towards the peripheral retina. • In severe cases retinal haemorrhage may be seen around the disc. • The term papilloedema is often, incorrectly, used to describe optic disc swelling. “Papilloedema” is swelling of the optic disc due to raised intracranial pressure.
Causes • Space occupying lesions including intracranial malignancy, subdural haematoma, and cerebral abscess. • Subarachnoid haemorrhage (commonly associated with vitreous haemorrhage). • Chronic meningitis. • Idiopatic intracranial hypertension(IIH). • Malignant hypertension. • Ischaemic optic neuropathy.
Optic disc cupping Appearance • The physiological cup is in respect to the rest of the disc. • Retinal vessels kink sharply as they emerge over the rim of the cup. • Haemorrhage s may be present . Causes • Most commonly one of the various types of glaucoma.
Optic atrophy Optic Atrophy. Note the chalky white disc with discrete margins. Optic atrophy is a late finding with increased intracranial pressure. Appearance • Pale optic disc due to loss of nerve fibres in the optic nerve head. Cause • Ischaemic optic neuropathy. • Optic neuritis. • Trauma. • Optic nerve compression.
Retinal haemorrhage Appearance • The appearance of haemorrhage depends on its location within the various layers of the retina. Deep haemorrhages appear as “dots” due to the close packing of the cells in this region. More superficial haemorrhages in the nerve fibre layer appear as more widespread “blotches”.
Causes Many pathological processes including: • Diabetes mellitus. • Hypertension. • Subarachnoid haemorrhage. • Blood dyscrasias. • Systemic vasculitis. • Valsalva related. • Trauma. • Bacterial endocarditis (known specifically as Roth spots).
Central/branch retinal artery occlusion Appearance • Large area of ischaemic white retina associated with sudden catastrophic visual loss. • Calcific, cholesterol or fibrin-platelet emboli can often be seen occluding the retinal artery/branch. Causes • Either embolic or thrombotic (remember giant cell arteritis also).
Central/branch retinal vein occlusion Appearance • Large widespread flame shaped haemorrhages classically giving the fundus a “stormy sunset” appearance. Associated with gradual onset painless blurred vision and visual loss. • Optic disc swelling may be present. Causes • Blood dyscrasias. • Diabetes mellitus. • Glaucoma.
Foster-Kennedy syndrome • Appearance • Unilateral optic atrophy. • Contralateral papilloedema. • Central scotoma • Anosmia (variable). • Systemic symptoms such as headache, dizziness, vertigo, and vomiting. • Causes • Meningioma of optic nerve, olfactory groove or sphenoid wing. • Frontal lobe tumour.
Pupillary examination • Examine the pupils for shape and symmetry • Ask the patient to fix the eyes on a distant point • Bring torchlight from the side to shine on the pupil • Look for constriction of that pupil (direct light reflex) and for the constriction of the opposite (consensual light reflex) • With the patient’s vision fixed on a distant point, present an object about 15 cm in front of the eyes and ask to focus on it (convergence) • Look for pupil constriction (accommodation reflex)
The 3rd ( oculomotor), 4th (trochlear), and 6th ( abdunces) nerves are considered together as their primary function is to provide motor innervation to the extrinsic muscles of the eye. Connections exist with the horizantal gaze centre in the pons and the vertical gaze centre in the midbrain.
Applied anatomy: III Motor: levator palpebrae superiors, superior rectus, medial rectus, inferior rectus, inferior oblique. (All the extrinsic muscles of the eye except the lateral rectus and superior oblique). Autonomic: parasympathetic supply to the constrictor (sphincter) pupillae of the iris and ciliary muscles. The main oculomotor nucleus lies anterior to the aqueduct of the midbrain. TheEdinger-westphal nucleus (accessory parasympathetic nucleus) lies posterior to the oculomotor nucleus. Fibres pass anteriorly, through the cavernous sinus and enter the orbit through the superior orbital fissure.
Complete CN III palsy. The affected eye assumes a "down and out" resting ...
Applied anatomy:IV • Motor: superior oblique The nucleus lies just inferiorly to that of the oculomotor nerve and has connections with the cerebral hemispheres, visual cortex and nerves III,IV, and VIII. Its fibres pass posteriorly and immediately cross one another. They then travel through the cavernous sinus, entering the orbit through superior orbital fissure.