Cranial Nerves
Cranial Nerves. Cranial Nerves. Cranial Nerves. Cranial Nerves. Mnemonic Aids for Cranial Nerves. On Old Olympus Towering Tops A Famous Vocal German Viewed Some Hops

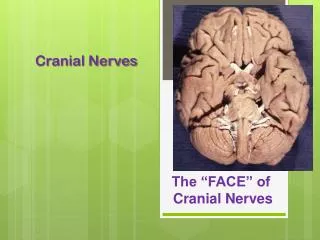
Cranial Nerves
E N D
Presentation Transcript
Mnemonic Aids for Cranial Nerves • On Old Olympus Towering Tops A Famous Vocal German Viewed Some Hops • Olfactory, Optic, Oculomotor, Trochlear, Trigeminal, Abducens, Facial, Vestibulocochlear, Glossopharyngeal, Vagus, Spinal Accessory (Accessory), Hypoglossal • Oh. Oh. Ooh...To Touch And Feel Very Green Vegetables...A H !!! • Oh, once one takes the anatomy final- very good vacations are heavenly!
Mnemonic Aids for Cranial Nerves • OLd • OPie • OCcasionally • TRies • TRIGonometry • And • Feels • VEry • GLOomy • VAGUe • And • HYPOactive
Mnemonic Aids for Cranial Nerves • Some Say Marry Money, But My Brother Says Big Business Matters More • The first letter of each word signifies whether the particular cranial nerve is sensory only (S); motor (M); or both sensory and motor (B)
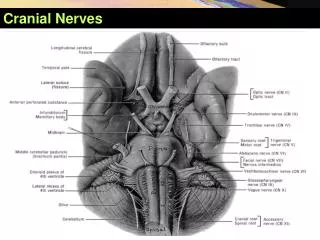
CranialNerves • Indicated by Roman numerals I-XII from anterior to posterior • May have one or more of 3 functions • Sensory (special or general) • Somatic motor (skeletal muscles) • Parasympathetic (regulation of glands, smooth muscles, cardiac muscle) • Proprioception • Positional information of body parts
Modalities- Sensory • GSS (GSA):General Somatic Sensory: • General senses from ectoderm (skin) • Pain, temperature, pressure, vibration, and proprioception • SSS (SSA):Special Somatic Sensory: • Special senses derived from ectoderm: • Sight, sound, balance. • GVS (GVA):General Visceral Sensory: • General sensation from viscera • SVS (SVA):Special Visceral Sensory: • Special senses derived from endoderm: • Taste and smell
Modalities- Motor • GSM (GSE):General Somatic Motor: • Skeletal muscles. • GVM (GVE):General Visceral Motor: • To smooth muscles of gut tract, glands, vessels, and all other internal organs • General visceral motor is autonomic motor. • SVM (SVE):Special Visceral Motor: • Muscles derived from pharyngeal arches. • Masticatory muscles • Muscles of facial expression • Pharyngeal muscles • Laryngeal muscles • Tongue muscles
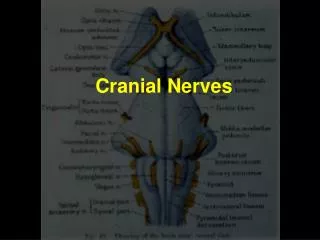
Generalizations • Cranial nerves have same basic structure as spinal nerves. Dorsal root and ventral root. Dorsal root ganglion. • Motor components of cranial nerves begin within brain within motor nuclei. Comparable to spinal cord anterior horns. • Cell bodies of sensory fibers are located in dorsal root (cranial) ganglia.
Generalizations • Special sensory cranial nerves: Are actually tracts. No motor nuclei and no sensory ganglia. • Motor cranial nerves: Begin in cranial motor nuclei. Have no sensory roots and no sensory root ganglia. • Mixed cranial nerves: Have both cranial motor nuclei and sensory ganglia. Sensory ganglia are usually given specific names.
Generalizations • For each cranial nerve know: Modality (modalities). Function (functions). Sensory areas and/or muscles innervated. Foramen through which it passes. Specific ganglion (if applicable). Specific information included in this slide presentation.
CranialNerves • Special Sense Nerves • I,II,VIII • Somatic Motor Nerves • Eye: III,IV,VI • Tongue: XII • “Rest of body” nerves • IX,X,XI • Face and jaws • VII, V
SENSORY SpecialGeneral Smell skin Vision teeth Hearing eye Taste tongue Balance oral cavity nasal cavity middle ear throat meninges MOTOR Muscles Glands eyes salivary extrinsic sweat intrinsic lacrimal jaws mucous larynx tongue throat ear facial expression Nerve “Targets” in Head
NERVE TARGET ENTER to CRANIAL CAVITY I. Olfactory Olfactory epithelium Cribiform plate (ethmoid) II. Optic Retina Optic canal (sphenoid) VIII. Auditory Inner ear Internal auditory meatus (temporal) Special Sense Nerves
Olfactory Nerve (CNI) • The receptors cells for smell form a patch of epithelium of about 5cm2(olfactory mucosa) in the roof of the nasal cavity. • It covers part of the superior nasal concha and septum.
Olfactory Nerve (CNI) • Olfactory receptor cells are neurons with a modified dendrite consisting of a swollen tip bearing 10-20 ciliacalled olfactory hairs. • The hairs are immobile and have binding sites for odor molecules. • The basal end of the cell tapers to become an axon. • These axons collect into small fascicles that leave the nasal cavity through pores (cribriform foramina) in the ethmoid bone • Collectively, the fascicles are regarded as cranial nerve I (olfactory nerve)
Olfactory Nerve (CNI) Fascicles emerging through the cribriform foramina
Olfactory Nerve (CNI) • Olfactory cells have a life span of approximately 60 days. • They are continually replaced by the differentiation of the basal cells into new olfactory cells. • They are the only neurons in the body directly exposed to the external environment.
Olfactory Nerve (CNI) • The tracts follow a pathway leadingto the medial side of the temporal lobe. • Input goes to the amygdala and hypothalamus which triggers emotional and visceral responses. • Olfactory signals differ from other sensory inputs in that they reach the cerebral cortex without passing through the thalamus
Optic Nerve (CN II) • Originates from the bipolar cells of the retina which are connected to the specialized receptors in the retina (rod and cone cells). • Electrical signals generated by the bipolar cells are transmitted to the brain through the optic nerve.
Optic Nerve (CN II) • The optic nerve exits the back of the eye in the orbit and enters the optic canal and exits into the cranium. • It enters the central nervous system at the optic chiasm (crossing) where the nerve fibers become the optic tract just prior to entering the brain.
Optic Nerve (CN II) • Most of the axons of the optic nerve terminate in the lateral geniculate nucleus (primary visual processing unit of the thalamus, integrates messages from two eyes into a single picture). • Information is then relayed to the primary visual cortex in the occipital lobe and superior colliculus (eye movement) from where spinotectal reflexes are mediated. optic tract optic radiation
Optic Nerve (CN II) • Begins in ganglionic layer of retina (not rods and cones). • Exits orbit through optic canal. • 50% decussation in optic chiasma: • Near pituitary gland • Near internal carotid • Modality: • SSS
Vestibulocochlear Nerve (VIII) • Composed of two branches that arise within the inner ear. • Vestibular branch arises from the vestibular organs of equilibrium and balance. • Relays afferent information related to the position and movement of the head • Cell bodies of vestibular nerve are located in the vestibular ganglion.
Vestibulocochlear Nerve (VIII) • Cochlear branch arises from the Organ of Corti in the cochlea and is concerned with hearing. • Cell bodies of cochlear nerve are found in spiral ganglion to the cochlear nuclei within the medulla oblongata.
NERVE TARGET EXIT CR. CAVITY IV. Trochlear Superior oblique m. (with trochlea) Sup. orbital fissure (sphenoid) VI. Abducens Lateral rectus “ III. Oculomotor (Also parasympathetic to ciliary mm, constrictor pupillae) • Sup.,med.,inf.rectus • Inferior Oblique • Levator palpebrae • superioris “ XII. Hypoglossal Intrinsic, extrinsic mm. of tongue Hypoglossal canal (occipital) Somatic Motor Nerves(Eye Muscles and Tongue)
Oculomotor Nerve (CN III) • If this nerve is damaged, the action of the remaining two muscles (superior oblique and lateral rectus) pulls the eye "down and out". • The nucleus is located medially in the midbrain, and the nerve fibers exit ventrally, just inside the peduncles.
Edinger-Westphal Nucleus • Source of the parasympathetics to the eye, which constrict the pupil and accommodate the lens. • It is located just inside the oculomotor nuclei. • The fibers travel in the IIIrd nerve, so damage to that nerve will also produce a dilated pupil.
Damage to Oculomotor Nerve • Lateral strabismus, as medial rectus is paralysed and the lateral rectus is unopposed; • Diplopia, double-vision as one of the eye deviates from the midline; • Inability to move the eye medially or vertically; • Ptosis as the ipsilaterallevatorpalpebraesuperioris is paralysed; • Mydriasis (dilated pupil of affected side) and unresponsiveness to light as the sphincter pupillae is non-functional and the dilator pupillae is unopposed; • Inability for the affected eye to focus on near objects as the ciliary muscles have also been paralysed.
Damage to Oculomotor Nerve Lateral strabismus (misaligned eye) Diplopia (double vision) Mydriasis (dilated pupil)
Trochlear Nerve (CN IV) • "Trochlea" is from the Latin word for pulley. • Supplies the superior oblique muscle. • Its cell bodies are located in the contralateral trochlear nucleus. • The trochlear nerve is unique in that: • It is the only cranial nerve attached to the dorsal aspect of the brainstem (exits the brainstem dorsally). • It is the only one to originate completely from the contralateral nucleus (The fibers cross over each other just like a half-tied shoelace in the roof of the fourth ventricle). Origin: midbrain Termination: Superior oblique Cranial passage: Superior orbital fissure
Clinical Significance of the Trochlear Nerve • Damage to the trochlear nerve result in much less drastic and noticeable deficits than damage to the oculomotor or abducens nerves. • The superior oblique muscle helps to move the eye downward and medially (inferomedial). • Attempted movements in these directions (e.g., reading or walking down stairs) may cause diplopia. • Eye points superolaterally
Clinical Significance of the Trochlear Nerve • Function: eye movements and proprioception • Clinical test for injury: ability to rotate eye inferolaterally • Effects of damage – double vision, patient tilts head toward affected side
Abducens Nerve (CN VI) • Enters orbit through superior orbital fissure. • Lies on medial aspect of lateral rectus muscle. • Innervates lateral rectus muscle of the eye. • Modality: • GSM.
Abducens Nerve (CN VI) • Clinical Significance of the Abducens Nerve (Lateral Gaze) • This causes medial strabismus (the affected eye deviates medially by the unopposed action of the medial rectus muscle). • The individual may be able to move the affected eye to the midline, but no further, by relaxing the medial rectus muscle.
Abducens Nerve Damage (CN VI) Medial strabismus
Abducens Nerve Damage (CN VI) Medial strabismus
Hypoglossal Nerve (CN XII) • Exits cranial cavity via hypoglossal foramen. • Descends anteriorly in neck between internal carotid and internal jugular. • In neck gives rise to superior root of ansa cervicalis and a nerve to thyrohyoid muscle. • Supplies extrinsic and intrinsic muscles of tongue. • Modality: GSM.
Hypoglossal Nerve (CN XII) • Is a mixed nerve. • The motor fibres arise from the Hypoglossal nucleus of the medulla oblangata • innervate both the extrinsic and intrinsic muscles of the tongue. • fibres are distributed to the hypoglossus, styloglossus, geniohyoid and genioglossus muscles and all the intrinsic muscles of the tongue • The intrinsic muscles of the tongue alter the shape of the tongue, while the extrinsic muscles alter its shape and position. • The genioglossus muscle protrudes the tongue. • The sensory root arises from proprioceptors within these same muscles.
Examination of the Hypoglossal Nerve • Trauma to the Hypoglossal nerve would result in difficulty speaking, swallowing, and protruding the tongue. • Ask the patient to stick out their tongue and to move it from side to side. The tongue will normally protrude from the month and remain midline. Note any deviations of the tongue from the midline. • Listen to the articulation of the patient's words.
Hypoglossal Nerve (CN XII) C1--first cervical nerve hf--hypoglossal canal