Cranial nerves
700 likes | 3.7k Vues
Cranial nerves. provide motor and sensory innervation for the head and neck damage of motor neurons results in cranial nerve palsy (central or peripheral?) motor pathways for cranial nerves are composed of how many neurons? where are they located?. Cranial nerve palsy.

Cranial nerves
E N D
Presentation Transcript
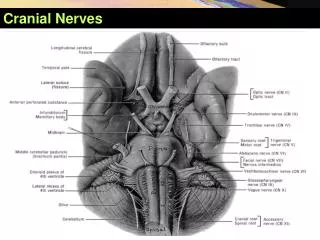
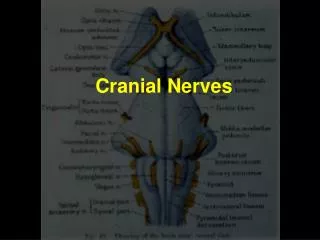
Cranial nerves • provide motor and sensory innervation for the head and neck • damage of motor neurons results in cranial nerve palsy(central or peripheral?) • motor pathways for cranial nerves are composed of how many neurons? • where are they located?
Cranial nerve palsy • The upper motor neuron – lesion results in an upper motor neuron weakness, central palsy • in: cortex, internal capsule, or brain stem above the nucleus • The lower motor neuron – lesion results in an lower motor neuron weaknesss, peripheral p. • in: the nucleus in the brain stem (the cell bodies form nuclei), or in any lower part of the cranial nerve
Olfactory nerve disorders • hyposmia/anosmia: bilateral and transient – rhinitis • unilateral: • damage of the fila olfactoria – through cribriform plate of the ethmoid bone head trauma - skull fractures • olfactory bulb and tract damage – tumours – meningeoma, glioma • uncinate fits – olfactory hallucinations (unpleasant) lesion in the olfactory cortex (uncus gyri hippocampi) – tumour - glioblastoma
Olfactory nerve examination • Testing the ability to smell or to identify different smells: • each nostril separately • the patient tries to identify the odor with eyes closed • recommended: perfume (flowers), spice (cinnamon, peppermint…), coffee, tobacco, soap… • avoid substances which irritate the trigeminal nerve (ammonia, vinegar…)
Optic tract and manifestations of its damage • the ocular systém reverses the image • optic chiasma – partial decussation • damage anterior to the chiasma: • scotoma • monocular blindness • lesion at the chiasma: • heteronymous hemianopsia • damage posterior to the chiasma: • homonymous hemianopsia • lesion in the optic radiation: • quadrantanopsia • lesion to the visual cortex: • one side – homonymous hemianopsia • bilateral – cortical blindness Mumenthaler
Optic nerve examination • visual acuity • optic fundus and disc: • papilloedema – prominence is measured in dioptres • in increased intracranial pressure (brain tumour?) • contraindication of lumbar punction! • visual fields – gross testing by confrontation
Impaired ocular movement 1 • Disorders of gaze (supranuclear, central), or conjugate deviation of the eyes: • horizontal • the frontal lesion – tonic deviation of the eyes towards the lesion Lindsay
Impaired ocular movement 2 • Disorders of gaze (supranuclear, central), or conjugate deviation of the eyes: • horizontal • the pontine lesion – tonic deviation away from the lesion Lindsay
Impaired ocular movement 3 • Disorders of gaze • vertical • upward gaze and convergence are lost • in midbrain tectum lesion = Parinaud´s syndrome Netter
Impaired ocular movement 4 Lesions of the cranial nerves (peripheral palsy): • III (oculomotor) • IV (trochlear) • VI (abducens) • with paralytic strabismus • with double vision (diplopia)
Oculomotor palsy • ptosis (levator palpebrae m.) • divergent strabismus(the affected eye deviates laterally) • paralysis of the eye movements and accommodation • pupil dilatation (mydriasis), • reaction to light is absent
Oculomotor palsy - paralysis of the eye movements (left eye)
divergent strabismus mydriasis paralysis of the eye movements Oculomotor palsy (on the right side) Perkin
Trochlear palsy • rare • weakness of downward gaze • double vision when looking downwards • the head may tilt to the opposite side to minimise the diplopia • diplopia is vertical Right fourth nerve palsy, the paretic eye turns up- and outwards; head tilting
Abducent palsy convergent strabismus failure of abduction on the affected eye (on looking to the paralysed side) horizontal diplopia Left sixth nerve palsy (looking to the left)
III, IV, VI cranial nerve examination • palpebralfissures (symmetrical? ptosis?) • positionofthebulbs (parallel? strabismus convergentordivergent?) • ocularmovements (full range? limitations?) • nystagmus (direction? degree?) • pupils: shape, size in mm (dilated – mydriasis, constricted – miosis) equality (isocoria? anisocoria?) reaction to light (light reflex): direct and consensual nearreactionto accommodation and convergence
Trigeminal nerve disorders • the fifth nerve: • sensory fibres subserve facial sensation (half of the face, 3 divisions) • motor fibres (in the mandibular division) innervate the muscles of mastication (masseter, pterygoids and temporalis) • disorders: • sensory loss • muscle weakness, atrophy (in peripheral palsy) • neuralgia
Trigeminal nerve examination • pressure to pointswherethedivisionsemerge –painful • sensation (eachdivisionseparately) for • pain • temperature • lighttouch • corneal reflex – blink response (trigemino-facial r.) – symmetrical? • masseter reflex (jaw jerk) • motor functionofthemasseter, temporal and pterygoidmuscles
Facial palsy • uppermotor neuron lesion, central paralysis: the upper branch is less affected (because the rostral part of the nucleus is innervated bilaterally) paralysis is marked on the muscles in the lower half of the face, on the opposite side • lower motor neuron lesion, peripheral paralysis: paralysis of all facial muscles on the same side Mumenthaler
Facial palsy Central
Facial palsy Peripheral: • the upper branches • flattened wrinkles on the forehead • lagophthalmos an attempt to close the eyes - the one eye does not close • Bell´s phenomenon the eyeball rotates upwards
Facial palsy Peripheral: • the lower branches • flattening of nasolabial fold • mouth angle drop • asymmetrical: • smile • showing teeth • purse lips
Facial nerve examination • observation • testing of the upper branches: • to wrinkle forehead (raise eyebrows) • to frown • to close eys tightly (persisting fissure in mm) • to close eyes against the resistance • testing of the lower branches: • to smile • to show one´s teeth • to purse the lips up • to blow out the cheeks • to whistle
Vestibulocochlear nerve disorders • Auditory function - hearing loss • Vestibular function: • vertigo(an illusion of rotatory movement), vomiting… • nystagmus(a rhythmical oscillation of the eyes) • a slow drift in one direction, followed by a fast corrective movement • nystagmus direction – in terms of the fast phase • horizontal, vertical, rotatory, diagonal, mixed… • nystagmus: grade I, II, III • tonic deviations • towards the damaged side • in peripheral vestibular lesions – „harmonious“ vestibular sy • dependence on the head position
Examination - tonic deviations • Hautant´s test – deviation of the arms - in angular degrees • Barány´s pointing test • (Unterberger gait test, stepping, marching test) • Romberg´s test • dependence of the fall direction on the head position • vestibular ataxia – gait with the eyes closed – deviation from the straight direction
Disorders of the lower cranial nerves Lesions of the cranial nerves (peripheral palsy): • IX (glossopharyngeal) mixed • X (vagus) mixed • XI (accessory) motor • palatal weakness - bilateral – nasal quality of speech • pharyngeal weakness - bilateral – dysphagia • vocal cord paresis – hoarseness of the voice or dysphonia • the shoulder is dropped • the patient cannot turn the head to the healthy side
IX, X, XI cranial nerve examination • swallowing difficulty? • assess the soft palate • at rest (symmetrical? palatal arch is drooped?) • during phonation (elevation?) • gag reflex (pharyngeal) – symmetrical? • accessory nerve (external branch): • sternomastoid muscle • trapezius muscle Lindsay
Hypoglossal paralysis and examination • paralysis: • upper motor neuron paralysis • tongue deviates opposite to the lesion • mild weakness • lower motor neuron paralysis • tongue deviates to the side of the lesion • atrophy • fasciculation • examination: • inspection • mobility of the tongue Lindsay
Bulbar and pseudobulbar palsy bulbar (nuclear) pseudobulbar (supranuclear) bilateral lesion of cortico-bulbar tract upper motor neuron lesion, central palsy dysarthria, dysphagia, n.VII,V masseter reflex increased emotional lability (unprovoked crying or laughing) frontal type of the gait cause: cerebrovascular disease, arteriosclerosis (multi-infarct conditions) • bilateral affection of the lower cranial nerves IX-XII or their nuclei in the oblongata • lower motor neuron lesion, peripheral palsy • dysarthria, dysphagia, n.VII,V • masseter reflex absent • tongue atrophy, fasciculations • cause: polyradiculoneuritis - Guillain-Barré syndrome), brainstem lesions – tumours, meningoencephalitis, motor neuron disease