Download
1 / 21
210 likes | 357 Vues
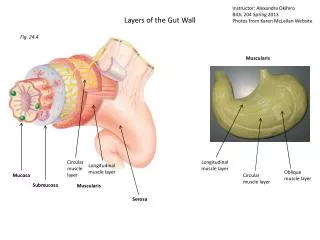
Mechanical vascular and neoplastic abnormalities of the gut. Intestinal obstruction. Hernia – protrusion of all or part of an organ from the cavity normally containing it. Trapping leads to oedema and obstruction of vascular supply

E N D
Intestinal obstruction • Hernia – protrusion of all or part of an organ from the cavity normally containing it. Trapping leads to oedema and obstruction of vascular supply • Volvulus – twisting of a loop of bowel about its mesentery. Commonest in sigmoid colon. Very common in Africa (associated with high fibre diet). Can be associated with worms. Leads to ischaemia/infarction
Intestinal obstruction • Adhesions – fibrous bans representing organised inflammation (after peritonitis, surgery) – internal hernias • Intussusception – telescoping of one segment of bowel into a more distal one
Intussusception • Occurs in infants and children (often associated with infection and lymphoid hyperplasia • In adults usually associated with a tumour
Vascular disorders • Ischaemic bowel disease • The bowel has a good collateral circulation but • Occlusion of a major vessel will lead to extensive infarction • Gradual loss of supply may be tolerated
Causes • Arterial occlusion – atherosclerosis, embolism, vasculitis • Venous occlusion – thrombotic states (malignancy, sepsis, dehydration) • Non-occlusive ischaemia – severe drop in blood pressure (cardiac failure, shock)
Extent and effects of injury • Mucosal necrosis only – can recover • Deeper necrosis leads to fibrosis and stricture • Transmural necrosis (gangrene) - perforation
Ischaemia • Chronic ischaemia can lead to ulceration, fibrosis and obstruction mimicking inflammatory disease
Intestinal neoplasms • Small intestine accounts for 75% of length of GI tract but is not a common site for tumours • Large bowel tumours are more common – particularly in the developed world
Small intestine • Carcinoid tumours are as common as adenocarcinomas • Other tumours include lymphoma, GIST Carcinoid with node metastases
Colon and rectum • Polyps (mass lesion protruding from a mucosal surface) are common: • Hyperplastic • Inflammatory • Adenomas (benign tumours of glandular epithelium) – important as precursors of cancer
Important Points • The adenoma-carcinoma sequence • Colorectal cancer as a model of multistage carcinogenesis in the human • Pathological determinants of patient prognosis
The adenoma-carcinoma sequence • Adenomatous polyps are common. How do we know that they predispose to cancer?…….and how do we assess the risk for a particular individual with a polyp(s).
Adenoma-carcinoma sequence 2 • Familial Adenomatous Polyposis Coli (hundreds of adenomas, certainty of cancer at an early age) • Anatomical distribution of adenomas and cancers is the same • Epidemiology is similar
Biology (a well studied system!) • A number of gene and chromosomal abnormalities have been identified (APC, p53, K-ras, loss of 18q, gain of 13q, 20)
Dukes’ Staging • A - confined to bowel wall • B - local spread beyond bowel wall • C - lymph node metastases
Dukes’ Staging and Prognosis • A 90% 5yr survival • B 70% 5yr survival • C 30% 5yr survival
Other colonic neoplasms • Lymphoma • Carcinoid • GIST