Download
1 / 43
490 likes | 1.17k Vues
Complications following Strabismus surgery. F.Fazel :MD. Disease Entity .

E N D
Complications following Strabismus surgery F.Fazel :MD
Disease Entity • Strabismus surgery is typically recommended when a patient’s eye alignment can no longer be treated with conservative measures such as eyeglasses, eye patching, prisms, and orthoptic exercises. Like many other ophthalmic procedures, strabismus surgery is very safe and effective, but complications can occur and need to be diagnosed and treated early to optimize post-operative outcome.
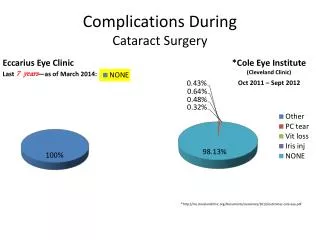
Complications • Unsatisfactory eye alignment is the most common complication. Despite careful pre-operative measurements and utilization of common surgical dosage tables, a certain percentage of patients will be overcorrected or undercorrected after. Change in the refraction can occur, especially if twomuscles are operated in the same eye. For example, operating on two horizontal muscles can induce a small with-the-rule astigmatism This change is temporary and resolves after a few months.
Complications • Diplopiacan occur, particularly in adult patients that are overcorrected. Patients younger than age 10 typically can suppress the deviated eye, but older patients may not have suppression or, if suppression is present pre-operatively, may not be able to shift the suppression scotoma to cover an overcorrection. • Scleral perforation can occur from an inadvertent deeppass of the suture needle or during dissection to isolate and disinsert the muscle tendon, particularly in the presence of scarring during a re-operation. In most cases, the perforation does not create a problem other than a chorioretinal scar, but in some cases can trigger endophthalmitis, vitreous hemorrhage, or retinal detachment.
Complications • Post-operative infection can occur, usually within the first week after surgery. Most infections occur around the initial surgical incision into the conjunctiva.Suture abscess localized to knot may occure. Rarely infections can penetrate deeper into the orbit with proptosis, eyelid swelling, chemosis and erythema in the classical presentation of orbital cellulitis,and sometimes endophthalmitis can develop, either with or without a scleral perforation. • Allergic reactions can occur in response to either the suturematerial or post-operative medications. Sometimes, these reactions can be difficult to distinguish from post-operative infections since they tend to occur in the same time frame. Some patients present late with increasing inflammation and discomfort; infection and allergic reaction should be considered in this situation as well.
Complications Foreignbodygranuloma can develop, usually a few weeks after surgery. The granuloma typically presents at the suture site as a localized, elevated, hyperemic mass that is less than 1 cm in diameter • Conjunctival inclusion cyst can present days to years after surgery. This translucent subconjunctival mass occurs when conjunctival epithelial cells are buried beneath the conjunctival surface during surgery.
Complications Conjunctival scaring can be a persistent problem after surgery. Instead of returning to the typical translucent white appearance, the conjunctiva can remain chronically hyperemic and pink, particularly after a second or third operation. This complication can be exacerbated by advancement ofTenon’s capsule too close to the limbus, particularly during a resection, or by advancement of the plicasemilunaris onto the bulbar conjunctiva. If severe, the conjunctival scarring itself can cause a restrictive strabismus. • Fat adherence can be cause by a violation of Tenon’s capsule with prolapse of orbital fat. The orbital fat can cause a fibro-fatty scar that is adherent to the muscle and globe, potentially leading to a restrictive strabismus.
Complications Dellencan occur on either the cornea or sclera when thickened bulbar conjunctiva (either from scarring, hemorrhage, or swelling) prevents adequate and even lubrication of the ocular surface. Fluorescein pools within the indentation of the cornea or sclera without creating true staining. • Anterior segment ischemia occurs when strabismus surgery creates impaired blood flow to the anterior segment. Most of the blood supply to the anterior segment flows through the ciliary arteries within the four rectus muscles. Simultaneous surgery on three rectus muscles in the same eye, or two rectus muscles in a patient with compromised blood flow from vascular disease, can cause ischemia. Typical findings in anterior segment ischemia include iritis, corneal edema, folds in Descemet’s membrane and, if severe, anterior segment necrosis and phthisis bulbi of the operated eye. • Eyelid retraction or ptosiscan be caused by strabismus surgery on the vertical rectus muscles. The eyelid retractors, particularly in the lower eyelid, are adherent to the intermuscular septum and fascial tissue around the vertical rectus muscles. This connection creates a shift in eyelid position during standard recession or resection surgery of the vertical rectus muscles.
Complications • Lost muscle occurs when the muscle slips free of the sutures or surgical instruments during surgery. This constitutes a surgical emergency and immediate surgical attempts to recover the muscle should be made. • Slipped muscle occurs when the sutures capture only the superficial muscular capsule instead of securing the muscle belly. Post-operatively, the muscle belly retracts within the muscle capsule, leading to clinical weakness of the operated muscle.
Etiology • Unsatisfactory eye alignment. It can also occur from pre-operative measurement errors of the eye misalignment, intra-operative measurement errors in extraocular muscle position, and excessive scarring or inflammation. Late causes of poor alignment can come from poor sensory adaptation to the new eye position. • Change in the refraction post-operatively occurs from a change in the force the extraocular muscle places on the cornea through its attachment to the sclera. Over time, this change in force usually reaches a new equilibrium, typically with restoration of the original corneal refractive shape. • Diplopia can occur in patients capable of vision in each eye from an imperfect eye alignment. Small amounts of residual vertical or torsional misalignments can be difficult to fuse into a single image, particularly if the misalignment is opposite to the pre-operative misalignment (overcorrection). Rarely, patients may have horror fusion,is, the inability to fuse despite well-aligned eyes.
Etiology • Scleral perforations can occur from an inadvertent deep pass of the suture needle, particularly if the sclera is thinned from a pathological change in eye structure, such as high myopia with a staphyloma. It may also occur when the suture is placed in the normally thinned sclera directly behind the muscle insertion. Perforations can also occur during the dissection, isolation, and disinsertionof the muscle tendon, particularly in the presence of scarring that may make exposure and isolation of the muscle tendon more challenging. • Post-operative infections can occur if sterile technique is violated or if the patient has a pre-existing condition such as blepharitis or nasolacrimalstenosisthat increases the bacteria count at the surgical site. • Allergic reactions occur sporadically in patients that are sensitive to the materials or medications used in the peri-operative period.
Etiology • Foreign body granulomasoccur sporadically in susceptible patients. The exact etiology is unclear, since the occurrence rate appears equal in primary and secondary surgeries and the existence of a prior granuloma does not appear predictive of subsequent granulomas. • Conjunctival inclusion cysts occur when conjunctivalepithelial cells are buried beneath the conjunctival surface during surgery. These cells can multiply over time to create a subconjunctival cyst days to years after the original surgery. • Conjunctival scaring is more common after a re-operation and also after a surgical resection, when advancement of the muscle belly may advance the thicker posterior Tenon’s capsule closer to the limbuswhere it is more visible.
Etiology Fat adherence is caused by violation of Tenon’s capsule with prolapse of orbital fat. It is more common with extensive posterior strabismus surgery • Dellenis more common after a limbal incision than a fornix incision, particularly in the presence of excessive scarring, swelling, or hemorrhage. They are more common after resectionsurgery than recession surgery. Any disruption of the tear layer on the sclera or cornea can create a dellen. • Anterior segment ischemia is more common in older patients with microvascular risks factors such as diabetes and hypertension. It also occurs more commonly in patients with extensive prior peri-ocular surgery,such as scleralbuckling, that can diminish anterior segment blood flow. Early recognition and treatment of ischemia with corticosteroids is necessary to minimize the chance of adverse consequences.
Etiology • Eyelid retraction or ptosiscan occur with any vertical rectusrmuscle surgery, but is more prevalent with largersurgicaldosages. Lost muscle is common when operating on the medial rectus and inferior rectus because of the shorter arc of contact. A lost muscle is more common with tight or contracted muscles because the increased passive tension increases the possibility of the muscle tendon pulling free of sutures or clamps during surgery. A lost muscle can occur in association with overall poor ystemic health. Pulled In Two Syndrome (PITS) can happen when a weakened muscle ruptures during surgery, typically at the junction between the muscle belly and tendon,resulting in loss of the posterior muscle belly. • Slipped muscles occur when less than full-thickness bites are used to capture the muscle tendon. Superficialsutures only incarcerate the muscle capsule, allowing the muscle belly to retract posteriorly when force is exerted during contraction.
Risk Factors Unsatisfactory eye alignment : patients with poor fusion potential and in patients with more complicated types of strabismus. Patients with dense amblyopiaor structural problems in one or both eyes have limited potential for binocular vision and will not employ fusional mechanisms to improve or maintain eye alignment. Similarly, patients with neuro-developmental anomalies have been shown to have higher rates of undercorrection and overcorrection after strabismus surgery. Also, patients with more unusual and severe forms of strabismus, such as 3rd nerve palsies, are more difficult to align satisfactorily with surgery. • Changeinrefraction:Operating on more than one muscle per eye, particularly utilizing larger amounts of recession or resection, can increase the risk of a change in refraction. Diplopia is increased inadultpatients who possess limited ability to suppress the second image. The risk is also higher in more complicated types of strabismus, particularly vertical, torsional, or paretic forms of strabismus. In those patients, it may be more difficult to create a useful area of single binocular vision.
Risk factors Scleral perforations is increased if the sclera is thinned and also if there is significant scarring or hemorrhage (more common during a re-operation) that may impedeexposureof the sclera for suture placement. The risk is also greater with very posterior suture placement, such as for posterior fixation sutures, because it is more difficult to visualize and place the suture at the proper depth in the sclera in the retroequatorial globe. • Infection is increased if the patient has a pre-existing condition such as blepharitis or nasolacrimalstenosis that increases the bacteria count at the surgical site. It may also be increased in very young patients, particularly those with developmental delay, that may have difficulty cooperating with hygiene and antibiotic eye drops after surgery. • Allergic reactions is increased in patients with a history of hypersensitivity reactions or systemic allergies or asthma. • Foreignbodygranulomaappears to be related to the suture material. With the elimination of gut suturesin most strabismus surgeries, granulomas have become uncommon.
Risk factors Conjunctival inclusion cyst is increased when the conjunctival wound is not closed meticulously. In particular, for fornix incisions, relying on simple apposition of the conjunctival wound without sutures appears to increase the risk of subsequent cyst formation. • Conjunctival scarring is increased for a re-operation and also after a surgical resection, when advancement of the muscle belly may advance the thicker posterior Tenon’s capsule closer to the limbus where it is more visible. Care must be taken to avoid creation of conjunctival foreshortening or symblepharon. • Fat adherence is increased with more posterior strabismus surgery, such as operating on the inferior oblique muscle, exploring posteriorly to retrieve a lost muscle, or dissecting more posteriorly to place a posterior fixation suture. • Dellen is higher for a limbal incision than a fornix incision, because the subsequent irregularity of the perilimbal • conjunctiva can cause a disruptin of the tear layer • in the anterior sclera and cornea.
Risk factors Anterior segment ischemia is higher when operating on multiple muscles in the same eye, in older patients with microvasculardisease, and in patients with prior extensive eye surgery that might also disrupt the ciliary vessels, such as scleral buckling procedures. • Eyelid retraction or ptosisis increased in subjects undergoing vertical rectus recessions or resection with high surgical dosages, particularly surgeries involving the inferior rectus. • Lost muscle increases with poor overall systemic health, with extensive scarring from prior eye surgery, and with surgery on a tight, contracted muscle. • Slipped muscle is increased when the muscle is tight, such as with dysthyroidorbitopathyor the contracted antagonist of a paretic muscle. A superficial suture pass is more likely to capture just the muscle capsule, and the tight muscle is more likely to retract within the muscle capsule after surgery.
Management • Optical treatments include a change in refraction, temporary or permanent prisms, or optical blur or occlusion. • Medical treatments include antibiotics – topical, systemic, or intravitreal – and anti-inflammatory medications, especially topical corticosteroids. • Surgical treatments include excisional biopsies, release of scar tissue, treatment of any retinovitreal disorders, and repeat strabismus surgeries.
Optical therapy • Optical therapy is directed at correcting any change in refractiveerror following surgery. Prisms may also be used in select cases to alleviate diplopia
Medical therapy Infections, topicalantibiotics are used to treat conjunctivitis, systemicantibiotics are used to treat preseptal and orbital cellulitis, and intraviteal antibiotics are used to treat endophthalmitis . Granulomas and conjunctival inclusion cysts, topical corticosteroids are used for several weeks, with possible surgical excision if no clinical response is observe. Allergies, the antibiotic eye drops should be changed, with the possible addition of a topical corticosteroid or antihistamine if the symptoms persist. Dellen formation, aggressive topical lubrication with artificial tears, sometimes in conjunction with eye patching, can help until the chemosis and swelling subside and the ocular surface becomes smooth again. Anteriorsegmentischemia, topical and systemic corticosteroids can relieve inflammation until collateral vascularization can occur.
Surgery • Lostmuscle, an attempt should be made to retrieve the muscle promptly, during the samesurgery if possible. If the muscle cannot be retrieved, a transpositionsurgery can be considered, although there is a risk of anterior segment ischemia by performing surgery on three eye muscles (the lost muscle plus two transposed muscles) at the same time. • Unsatisfactorypost-operativealignment may or may not require surgical correction. Sometimes prisms can be incorporated temporarily (fresnel prisms) or permanently into eyeglasses and further surgery deferred. In other situations, the prisms can be weaned slowly over time as fusional mechanisms build, allowing single binocular vision without prisms. Many cases of unsatisfactory eye alignment will need another strabismus surgery, particularly in the case of a slipped muscle or restrictive scarring where the eye alignment will not improve over time. • Scleralperforation may or may not require additional surgery. Most cases resolve without treatment, but the presence of infection, significant hemorrhage, or retinal detachment may require a vitrectomy or other surgeries as indicated. The use of cryotherapy or laserretinopexy at the time of perforation is controversial in the absence of retinal perforation.
Surgery • Foreignbodygranulomas and conjunctivalinclusioncysts may require excision if they are symptomatic and failtorespondt otopicalcorticosteroids. • Persistentconjunctivalscarring or a dellen may require surgery to remove scar tissue and smooth the conjunctival surface. • Eyelidretraction or ptosis may require oculoplasticsurgery to restore the normal lid configuration, particularly if the defect prevents proper eyelid closure or affects peripheral vision. • Lostmuscle can benefit from pre-operativeimaging to help locate the muscle. Depending on the location,a posterior orbital approach with the aid of an orbital surgeon can sometimes successfully isolate and retrieve the lost muscle. If the attempt to locate the muscle is unsuccessful, transposition surgery can be effec at restoring primary gaze alignment.
Prognosis • All of the complications of strabismus surgery, with the notable exception of endophthalmitis, have an excellent prognosis for recovery with proper treatment. Many of the complications lessen or disappear with time and conservative treatment, while others respond well to additional surgery. When severe, anteriorsegmentischemiacan progress to necrosis and phthisis bulbi, but most cases resolve with corticosteroids over time. Endophthalmitis, on the other hand, carries a significant risk of permanent vision loss even with prompt treatment.