Download
1 / 10
190 likes | 1.16k Vues
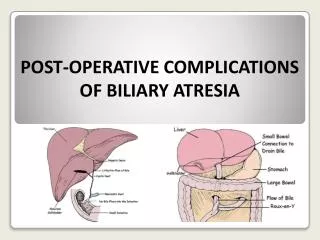
Complications of biliary surgery. Aswad Habeeb Hameed Al-Obeidy FICMS GE & Hep. Complications of biliary surgery. Include strictures, bile leaks, and sump syndrome The initial management of suspected bile duct injury must begin with diagnostic cholangiography

E N D
Complications of biliary surgery Aswad Habeeb Hameed Al-Obeidy FICMS GE & Hep
Complications of biliary surgery • Include strictures, bile leaks, and sump syndrome • The initial management of suspected bile duct injury must begin with diagnostic cholangiography • The type and extent of nonoperative intervention will be determined by the anatomic site of the bile duct injury
Strictures • The most common cause of a benign biliary stricture is prior biliary tract surgery • Cholangitis or jaundice resulting from a stricture is most likely to occur within 2 years of the original surgery • Surgical repair of a biliary structure is successful in 90% of cases • Is difficult in patients with multiple prior operations or an intrahepatic stricture
Strictures • Nonoperative therapy is indicated in patients for whom surgery poses a high risk or in whom a stricture is in a nonoperable site • Radiologic intervention consists of a combination of balloon dilation, external stenting with large-bore catheters (12 to 20 French), and, more recently, stenting with internal metal endoprostheses (24 to 30 French) • Long-term clinical improvement has been reported in several series in more than 50% of cases • In patients for whom initial surgical repair fails is somewhat lower, with a reported overall success rate of 30%
Strictures • Complications associated with metal endoprostheses include stent migration and occlusion due to mucosal hyperplasia within the stent • Patients with inoperable recurrent benign biliary stricture often need multiple biliary interventions • In these patients, repeated and convenient access to the biliary tree can be achieved via a jejunal loop that is surgically affixed to the abdominal wall
Strictures • Endoscopic intervention requires that a wire be negotiated through the stricture • Followed by dilation with a rigid (Sonde) dilator or a Grüntzig-type balloon, or both • The stricture is stented for a variable period. Second dilations may be necessary after removal of the stent • Some groups advocate endoscopic balloon dilation and stent placement for benign strictures, with excellent results (approaching 88%) after several years • long-term endoscopic stenting of a benign lesion only when an operative approach is unlikely to provide definitive therapy or is hazardous, as in patients with significant portal hypertension
Bile Leaks • Operative bile duct injury may lead to the development of a biliary leak (fistula) or biloma (bile collection) • Diagnostic cholangiography frequently reveals the location of the bile leak • If an extrahepatic biliary leak is detected, a nasobiliary catheter or stent may be placed across the disruption in the bile duct to divert bile temporarily from the site of injury and allow time for the injury to heal
Bile Leaks • If the bile leak is small, endoscopic sphincterotomy alone may permit spontaneous closure of the fistula • Alternatively, bile leaks may be treated with diversion of bile via a percutaneous transhepatic drainage catheter • The fistula does not resolve after simple biliary diversion, transcatheter occlusion techniques (e.g., sclerosis with tetracycline) may be used to close the leak
Sump Syndrome • Is an infrequent complication of a side-to-side choledochoduodenostomy • Stenosis of the surgical anastomosis occurs, and as food, stones, and other debris accumulate in the CBD distal to the stenotic anastomosis and proximal to the papilla, overgrowth of bacteria results in suppurative cholangitis
Sump Syndrome • Sump syndrome can be treated with a combination of endoscopic sphincterotomy and passage of a balloon through the distal CBD to sweep out debris from the duct • Alternatively, it may be possible to extract debris and stones via the choledochoduodenostomy, obviating a papillotomy • However, without a papillotomy and dilation of a strictured choledochoduodenostomy, the sump syndrome may recur