Download
1 / 23
230 likes | 509 Vues
DoH IVIG Workshop Update, neurology usage and outcomes measurement. Dr Michael Lunn National Hospital for Neurology and Neurosurgery Queen Square, London WC1N 3BG. Outline. Neurology IVIG usage update Neurology in 2011 Guidelines Update Measuring outcomes Update guidelines

E N D
DoH IVIG WorkshopUpdate, neurology usage and outcomes measurement Dr Michael Lunn National Hospital for Neurology and Neurosurgery Queen Square, London WC1N 3BG
Outline • Neurology IVIG usage update • Neurology in 2011 Guidelines Update • Measuring outcomes • Update guidelines • Measuring outcomes in clinical practice • What’s wrong with what we are using • How can we make it better?
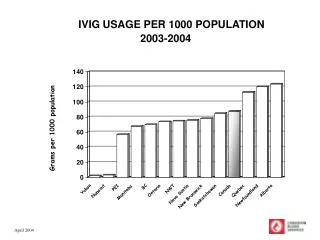
How inclusive is the database data now? • In 2009 PASA estimated only 60% data capture • GBS cases • 1.2-1.5 per 100000 • 720-900 cases • 60% require Rx • In 2009 260 GBS pts in database • Thus ?48 – 60% capture • In 2010 – 633 cases ?almost complete – 90%? 90.7% capture
This update did not review all of the Second Edition Guidelines content, but limited its focus to three key areas • defining selection criteria for appropriate use; • efficacy outcomes to assess treatment success; • reassignment of existing indications /inclusion of new indications.
Reassignment of existing indications /inclusion of new indications.
2009 • 24 patients with polymyositis • Some life threatening • >50% approved • Polymyositis likely to be immune mediated • IBM (previously black) • 2 cases only approved as exceptionality • Not infrequently ‘inflammatory’
Myositis criteria • Diagnosis of myositis by a neurologist, rheumatologist, immunologist of: • Patients with PM or DM who have significant muscle weakness; • OR Dysphagia and have not responded to corticosteroids and other immunosuppressive agents; • OR Patients with IBM who have dysphagia affecting nutrition (NOT patients with rapidly progressive IBM) • Outcomes and test dosage schedule suggested
Grey indications - changes • Immune-mediated disorders with limited evidence of immunoglobulin efficacy • Presumed immune-mediated disorders with little or no evidence of efficacy
Immune-mediated disorders with limited evidence of immunoglobulin efficacy • Acute disseminated encephalomyelitis • Autoimmune encephalitis (including NMDA and VGKC antibodies, among others) • Cerebral infarction with antiphospholipid antibodies • Chronic regional pain syndrome • CNS vasculitis • Intractable childhood epilepsy • Neuromyotonia • OpsoclonusMyoclonus
Immune-mediated disorders with limited evidence of immunoglobulin efficacy • Acute disseminated encephalomyelitis • Autoimmune encephalitis (including NMDA and VGKC antibodies, among others) • Cerebral infarction with antiphospholipid antibodies • Chronic regional pain syndrome • CNS vasculitis • Intractable childhood epilepsy • Neuromyotonia • OpsoclonusMyoclonus
Autoimmune encephalitis (including NMDA and VGKC antibodies, among others) and neuromyotonia • Granerod J et al 2009 – Lancet Infectious Disease • 203 patients with encephalitis in UK in 2006-2008 • 42% infectious, 21% autoimmune, 37% unknown • 16 case reports and small series of IVIG responsive Ab-mediated encephalitis since 2009
Complex Regional Pain Syndrome • Goebel A, Baranowski A, Maurer K, Ghiai A, McCabe C, Ambler G. • Intravenous immunoglobulin treatment of the complex regional pain syndrome: a randomized trial. • Ann Intern Med. 2010 Feb 2;152(3):152-8.
Presumed immune-mediated disorders with little or no evidence of efficacy • Acute idiopathic dysautonomia • Diabetic proximal neuropathy • PANDAS • Paraneoplastic disorders that are known not to be B- or T-cell mediated • POEMS
Measuring outcomes:Current practice, potential and future possibilities ‘This update provides efficacy outcomes to be measured in all indications…. Efficacy outcomes are expected to play an important role in the IAP decision-making process for patients……This change reflects the wider change of focus in the NHS to patient outcomes, as presented in The NHS Outcomes Framework.’