Sciatic Nerve Block
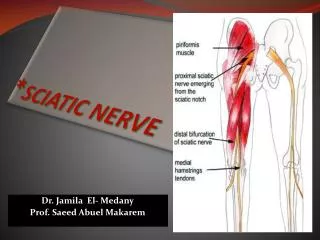
Sciatic Nerve Block . Tiffany Tavernier. L4-S3 spinal nerve roots Largest nerve trunk in the human body Distribution = hamstrings, long head of biceps femoris , adductor magnus ; part of hip and knee joint

Sciatic Nerve Block
E N D
Presentation Transcript
Sciatic Nerve Block Tiffany Tavernier
L4-S3 spinal nerve roots • Largest nerve trunk in the human body • Distribution = hamstrings, long head of biceps femoris, adductor magnus; part of hip and knee joint • Blocks skin of posterior aspect of thigh and entire leg below knee exception of skin of medial aspect of lower leg Some Basics….
Different Approaches.. • Classical Posterior Approach • Pt lies in lateral decubitus position • Landmarks: greater throchanter and posterior-superior iliac spine • Needle is inserted 4-5 cm distal to midpoint btw the two landmarks perpendicular to skin in all planes • Parasacral Approach • Pt lies in lateral decubitis position • Landmarks: posterior superior iliac spine and ischial tuberosity • Needle is inserted 6cm caudal to line btw the 2 in sagittal plane
Different approaches • Lithotomy • Pt is supine with hip flexed and upper leg perpendicular to torso • Landmarks: greater trochanter of femur and ischial tuberosity • Needle is inserted 4 cm in claudal direction midway between the 2 • Needle is advanced parallel to horizontal plane • Anterior approach • Pt is supine with legs extended • Landmarks: femoral crease and femoral arterial pulse • Needle inserted 405 cm distal from pulse of femoral artery and perpendicular to line of femoral crease
Posterior vs Anterior Approach • 100 pts undergoing minor knee surgery • Randomly divided by envelope to receive anterior or posterior approaches combined with femoral and lateral femoral cutaneous nerve blocks using US • 1% mepivacaine with short 1100m, 21 gauge • Block: 20mL of 1.5% mepivacaine with 1:400,000 epinephrine Anterior Approach • Nerve stimulator was used @ 2Hz to elicit foot plantar- or dorsiflexion Posterior Approach • Same as anterior, but without nerve stimulator.
Anterior vs Posterior Approach Measurements • both then placed in supine position with legs extended and femoral and lateral femoral cutaneous blocks were performed • Measurements of depth and size of sciatic nerve, needle depth, block execution time for sciatic nerve block, block execution time for all 3 blocks, time required for onset of sensory and motor blocks of sciatic nerve and duration of blockade of sciatic nerve were measured
Results • Sciatic nerve was located deeper in anterior approach • Both had similar block execution time for sciatic nerve block, but anterior approach took less time to complete all 3 blocks • Onset of sensory block for superficial peroneal, sural and tibial nerves was similar • Sensory block of posterior femoral cutaneous nerve was achieved less often with the anterior approach - less block of posterior area of thigh • Onset of motor block was similar with both approaches
Discussion • Although posterior femoral cutaneous nerve was rarely blocked with anterior approach, can still be used in knee surgery where thigh tourniquet is used pts who required fentanyl was similar btw groups tourniquet pain is not affected by presence of posterior femoral cutaneous nerve block