Download
1 / 20
230 likes | 325 Vues
Explore the acute viral fever, a leading cause of childhood deaths with severe complications. Learn about transmission, symptoms, and vaccination for effective prevention and control methods.

E N D
introduction • Acute viral exanthematous fever • Most contagious diseases known • Leading cause of childhood deaths in developing countries
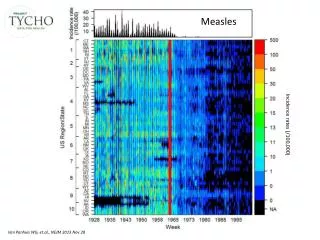
introduction • 6 million deaths of infants & children globally every year • Measles vaccination marked decline • Developed countries: estimated 20 million cases of measles resulted in 242,000 deaths in 2006
Agent • Genus morbillivirus • Family paramyxoviridae • Negative sense single stranded RNA virus • There is only one serotype.
Host • Susceptibility is universal • Most infections occur in 6months to 3years in developing countries • In india, >50% of cases were reported in children <5years of age
Host • Serious form in adults. • No gender predilection • Mortality higher in females at all ages • Immunity lasts lifelong • Nutritional status critical to decide severity • Persons with malnutrition, especially VAD or advanced HIV infection are at increased risk of severe or fatal measles.
Environment • In India, the peak incidence is in winter and early spring • In temperate countries most cases occur in winter months • Overcrowding favors transmission.
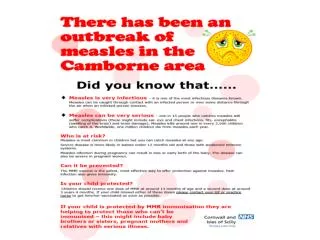
Transmission • Person to person by direct contact • Droplets or airborne spread of secretions • SAR ~ 90% • Communicability: 2 days before prodrome to 4days appearance of rash
Clinical Features • IP: ranges from 8 to13 days • 14 days from exposure to rash • Cough, coryza and conjunctivitis • Koplik’s spots: pathognomonic & towards the end of prodrome • Measles rash: 2 to 4 days after prodrome • First appears on the face and upper neck
Complications • Severe Diarrhea Dehydration, • Ear Infections : Otitis Media • Pneumonia (MCC Death) • Measles Encephalitis • SSPE • CFR:1-5% & 25% in SAM
Special Situations • Pregnancy: spontaneous abortion & premature delivery • May aggravate tuberculosis • Delay measles vaccination until after initiation of chemotherapy
Treatment • General nutritional support and • Treatment of dehydration with oral rehydration • Antibiotics • Ribavirin • Oral vitamin A administration
Prevention and Control • Active immunization is the primary method • Passive immunization: special circumstances. • General measures have little role
Active Immunization • A live attenuated vaccine • Edmonston B strain • single dose of 0.5 ml SC • two doses are given • Contraindication: Severely immunocompromised and pregnancy
Passive Immunization • Human Ig : 0.25 ml per kg • Within six days of exposure. • To susceptible household contacts like immunocompromised children
General Measures • Respiratory isolation • Exclusion from school for 1week from appearance of rash • Hospital strict isolation of cases • Articles soiled by secretions or fluids from vesicles to be incinerated or treated with disinfectants
Long Question : Discuss the epidemiology, treatment, prevention and control of Measles. • Short Note : (1) Complications of Measles (2) Measles vaccination