Download
1 / 98
1.03k likes | 1.31k Vues
Neoplasm: Biology of cancer & treatment modalities. By: Dr.Fatima M. Khajah. Neoplasm. Oncogenesis: pathogenesis of neoplasm. Carcinogenesis: pathogenesis of cancer. Oncogene: agent causing neoplasm. Carcinogene: agent causing cancer. Neoplasm. Tumor biology. Anti-tumor therapies.

E N D
Neoplasm:Biology of cancer&treatment modalities By: Dr.Fatima M. Khajah
Neoplasm • Oncogenesis: pathogenesis of neoplasm. • Carcinogenesis: pathogenesis of cancer. • Oncogene: agent causing neoplasm. • Carcinogene: agent causing cancer.
Neoplasm • Tumor biology. • Anti-tumor therapies. • Tumor markers.
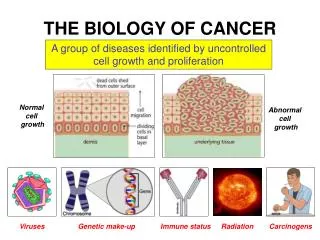
Tumor biology • Tumors are characterized by uncontrolled growth of transformed cells. • Tumors can be benign or malignant. • All tumors can be either classified as hematopoietic or nonhematopoietic in origin. • Within each category tumors can be further divided into those of : - Similar histologic origin (same organ), - Similar cell type ( e.g epithelial cell derived).
Tumor biology • The development of a tumor from a single transformed cell into metastatic tumor is categorized by stages and involves 3phases: 1- Initiation. 2- Promotion. 3- Progression.
Tumor biology 1- Initiation: - In which series of genetic mutations occur in sequence. 2- Promotion: - For initiated cells to become tumor cells, exposure to promoting agents or conditions is required. - The end of the promotion phase is characterized by the appearance of the first neoplastic cells. 3- Progression: - Invasive growth of the transformed cells and progression of the tumorous lesion into a highly metastatic tumor.
Tumor biology • How do tumors arise? - The formation of a tumor is a complex process primarily because tumors are not a single dx. (the progression toward the formation of a tumor requires multiple mutations that occur in sequence). - Cancer is multifactorial: mutations may be induced by: - External factors ( physical or chemical carcinogens) - Germ line mutations (Hereditary). - Combination of both. - Obscure causes.
Tumor biology • 1- External factors: - Responsible for most cancers in industrialized countries. - Includes: smooking, alcohol, some foods, exposure to sunlight and chemicals.
1- External factors: - Smoking: CA of bladder, lung, mouth, pharynx, larynx, osophagus. - Immunosuppression: Lymphomas. - Radiation: *X- rays & Gamma rays, atomic explosion: Leukemia. * radioisotopes: thyroid CA. - Chemical carcinogens: * Asbestos & polycyclic aromatic hydrocarbons: lung CA * Benzene: leukemia. * Aromatic amines: bladder CA. - Viruses: * HPV : cervical CA, * EBV : Burkitt’s lymphoma, nasopharyngeal CA. * Hep. B & C : hepatocellular CA.
Tumor biology • 2- Germline mutations: - This is due to inherited abnormal genes: * APC gene in FAP >>> adenocarcinoma colon. * Rb gene (C13) >>> retinoblastoma. * C17 >>> neuroblastoma. * Trisomy 21 in Down’s >> Leukemias in infants.
Tumor biology • 2- Germline mutations: - An example of germline mutation: colon CA. “ The morphologic changes from normal mucosa to early, intermediate, and late adenoma and finally to colorectal CA are associated with certain essential mutations that occur in sequence”
Tumor biology • Colonic tumorigenesis: • Tumorigenesis proceeds through a series of genetic alterations involving oncogenes ( ras ), and tumor suppressor genes ( particularly those on chromosomes 5q, 12p, 17p, and 18q). • The most commonly detected genetic alterations in colon cancer are the mutations and deletions of : - APC. - K- ras. - DCC. - p 53.
Tumor biology • Cellular transition occurs from normal colon epithelium to adenoma to invasive cancer. • APC mutations are believed to initiate tumor progression, with the development of other mutations as indicated in the diagram. Individuals with FAP inherit APC mutations and thus have already begun this pathway earlier than the general population. • The second important mutation may occur in the K-ras oncogene, which can produce ,through clonal expansion, a larger and more dysplastic tumor from the pre-existing small adenoma. (N.B: mutations in K-ras occur in about 50% of CA colon and in adenomas larger than 1 cm).
Tumor biology • Late adenomas and CA colon frequently show loss of the tumor suppressor gene DCC (deleted colon cancer or 18q) . Uncommon in early adenomas. • Finally deletion of the tumor suppressor gene p53 (17p) is observed in 75% of CA colon. Uncommon in adenomas. • Mutations in DCC and p53 are late events • Tumors continue to progress once CA have formed, and the accumulated loss of suppressor genes on additional chromosomes correlates with the ability of the tumor to metastasize.
Tumor biology • Multistep process: - Tumor initiation and progression results from stepwise accumulation of DNA mutations. - Several characters of malignant neoplasm are the result of multiple genetic defects. - Initial steps are reversible (dysplasia), but final malignant transformation is irreversible.
Initiation phase • Cell cycle: • Cell proliferation is a series of tightly controlled biochemical processes divided into interphase and mitotic (M) phase. • Interphase is further divided into 2 gap phases (G1 & G2), seperated by a DNAsynthesis phase (S). • Central to cell cycle progression are the cyclindependent kinases that bind to the cyclin proteins.
Initiation phase • Cell cycle is controlled by genes. • There are 4 main classes of regulatory genes: * Promotors: oncogenes. * Inhibitors: tumor- suppressor genes. * Genes regulating apoptosis. * DNA repair genes.
Initiation phase • Non-lethal genetic damage lies at the centre of carcinogenesis: - Promotors: Duplication. - Inhibitors: loss or damage. - Apoptosis genes: loss or damage. - DNA repair genes: loss or damage.
Initiation phase. • A critical point in cell cycle control is the transition from G1 to S. After passing this checkpoint, the cell is committed to division. • Tumor suppressor genes block G1 to S transision. • Oncogenes promote transition.
Tumor promotion • Stimulation of tumor development: - Even though tumors are characterized by unlimited growth, tumors are dependent on their environment for growth and development. - Tumor environment: - Stroma : parenchymal cells, epithelial cells, fibroblasts, endothelial cells, mast cells. - Immune cells: lymphocytes, polymorph, macrophages. - Basement membrane: forms the Extracellular matrix (ECM).
Tumor promotion • Stimulation of tumor development: - Together, tumor cells, ECM, stroma, and infiltrate produce factors (autocrine & paracrine) that, in cell-bound, matrix bound, or soluble forms, directly or indirectly influence tumor development. - Proliferating tumors invade neighboring cell populations, thereby breaking down boundaries designed to keep normal tissue architecture. - Tumor cells resistant to the regulatory signals can successfully expand into surrounding tissues.
Tumor promotion • Paracrine and Autocrine growth mechanisms: - Autocrine factors: promote growth of tumor cells themselves. - Paracrine factors: act on host cells or ECMs. - Tumor growth is dependent on the response of tumor cells to paracrine and autocrine factors. - These factors include: - Angiogenesis factors, growth factors, chemokines, cytokines, hormones, enzymes, cytolytic factors….. - Paracrine growth mechanisms are dominant during tumor initiation and promotion. Autocrine growth mechanisms become more prominent at later stages. - It is possible for a tumor to grow completely autonomous ( acrine state), independent of growth factors and inhibitors.
Tumor promotion Both stromal cells and infiltrate secrete paracrine factors that affect tumor development. Additionally, tumor cells secrete autocrine as well as paracrine factors that, in turn, act on stroma and infiltrating cells.
Tumor promotion • Role of inflammation in cancer: -. More recent work has demonstrated that infiltration in general has no proven prognostic values. - Recent data have confirmed that inflammation associated with chronic infections is a co-factor in carcinogenesis. - The tumor infiltrate include: macrophages, dendritic cells, neutrophils, eosinophils, mast cells, and lymphocytes. - Majority of tumor luecocyte infiltrate: Macrophages. - Majority of tumor infiltrating lymphocytes: T- lymphocytes.
Progression phase • Tumor progression: - The formation of tumor metastasis is characterized by detachment of some tumor cells from the primary tumor and infiltration into the blood stream or lymphatics (intravasation). - The reciprocal process occurs at other locations in the body (extravasation). - Both intravasation and extravasation are characterized by changes in the ECMs and their interactions with tumor cells. - Like tumor promotion, progression may also be dependent on infiltrates.
Progression phase • Outgrowth at prefferd sites: - Invasion & metastatic spread of tumor cells is not random. - Seal and soil hypothesis: Paget observed in 1889 that breast CA often metastasize to the liver, lungs, bones, adrenals or brain. He hypothesized that tumor cells ( the seed) would grow only in selective environments ( the soil) where conditions supported tumor growth. - Three major theories for soil: * Growth factor theory. * Adhesion theory. * Chemokines theory.
Neoplasm • Tumor biology. • Anti-tumor therapies. • Tumor markers.
Anti tumor therapies 1- Conventional: - Surgery:Excision of malignancy. - Chemotherapy:Drug- induced tumor cell lysis. -Radiation:Radiation induced tumor cell death 2- Alternative: - Oncoviral:Tumor cell lysis through selectively replicating virus. - Gene: Restore/add or inhibit expression of particular genes in tumor cells. - Antiangiogenesis: Blockade of tumor vasculature. - Immune: Tumor lysis through manipulation of the host’s immune system. - Stem cell: Graft versus malignancy response through stem cell transfer.
Anti tumor therapies • Chemotherapy. • Radiotherapy. • Alternative treatments.
Anti tumor therapies • Chemotherapy: - Localized tumors may be treated successfully by surgery or radiotherapy, but metastasis can only be cured by systemic treatment, which will normally be chemotherapy. - In addition, the combination of chemotherapy with surgery &/or radiotherapy may also increase local tumor control.
Anti tumor therapies • Chemotherapy: - Adjuvant chemotherapy: Chemotherapy given after surgery or radiotherapy to control the primary Dx. - Neo-adjuvant chemotherapy (primary chemotherapy): chemotherapy as an initial treatment used in localized but extensive CA, where the local control may be improved by combining 2 modalities of Rx. (e.g., large primary breast tumors). - Induction chemotherapy: chemotherapy used as a primary treatment for patients with widespread Dx.
Anti tumor therapies • Chemotherapy: - Goal: to kill rapidly dividing cells with drugs and leave other cells unharmed. - Unfortunately, certain normal cells also divide rapidly; including hair cells, bone marrow cells, and epithelial cells lining the digestive tract.
Anti tumor therapies • Chemotherapy: -Mechanism of action: 1-Most anticancer drugs cause DNA damage or inhibit DNA replication & transcription (cytostatic drugs). 2-In addition to the direct damage effects, certain genes may be triggered that are involved in apoptosis leading to cell death.
Apoptotic pathways: Chemotherapeutic drugs can induce apoptosis in tumor cells through a receptor-dependent (1) (extrinsic pathway) or receptor-independent (2) (intrinsic pathway). Both pathways induce release of cytochrome c from mitochondria, which triggers activation of various caspases in sequence, ultimately leading to apoptosis.
Anti tumor therapies • Chemotherapy: • Apoptosis: - Physiologic apoptosis appears to be regulated by multiple genes, but promotion of cell death by cytostatic drugs is usually regulated by a select number of genes. - These genes include both tumor suppressor genes such as p53, and oncogenes such as myc, E2F, c-jun, and bcl-2 (B-cell leukemia / lymphoma gene 2).
Chemotherapy: • Apoptosis: - p53 gene: - Induces growth arrest by blocking cell cycle progression from G1 to S phase to allow repair of the DNA. - If the repair is unsuccessful (as may be the case after Rx with certain drugs), the cells undergo apoptosis. - However, p53 is mutated in about 55% of tumor types, which may contribute to resistance to apoptosis – inducing drugs.
Chemotherapy: • Apoptosis: - myc & c-jun genes: - Both encode transcription factors that play a central role in regulating cell proliferation, differentiation and apoptosis. - E2F gene: - It is a family of transcription factors that promote S- phase entry and thus with respect to cell growth appears to have opposite function as p53.
Chemotherapy: • Apoptosis: - bcl-2 gene: - Is a member of a family proteins that inhibit apoptosis. - High levels of bcl-2 are found in tumor cells and may confer resistance to anticancer drugs. - Initially, dysregulation of bcl-2 was found in B-cell malignancies, but over expression has also been noted in solid tumors, including prostate, lung, colon, and stomach CAs.
Anti tumor therapies • Chemotherapy: • Apoptosis: ( in summary) - Cell cycle progression is under tight genetic control. - Growth factors or other stimuli activate oncogenes or inactivate tumor suppressor genes to allow progression through the cell cycle. - Cells that receive conflicting, excessive, or unbalanced mitogenic signals undergo apoptosis. - A similar deregulated cell cycle control and induction of apoptosis is observed after treatment with certain chemotherapeutic drugs.
Anti tumor therapies • The 4 main groups of chemotherapeutic drugs: - Alkylating agents. - Antimetabolites. - Vinca alkaloids. - Antimitotic antibiotics.
Anti tumor therapies • Alkylating agents: - Examples: cyclophosphamide, Chlorambucil. - Mechanism: They contain an alkyl group (e.g., CH3), which combines with other intracellular molecules such as nucleic acids, proteins (especially enzymes), and cell membranes. Damage to the enzymes which link DNA strands thus impairs mitosis during the S phase. - Side effects: nausea, vomiting, alopecia, neuropathy, nephropathy, ototoxicity, painful arm, flu-like, leukaemia.
Anti tumor therapies • Antimetabolites: - Examples: methotrexate, 5-flurouracil, 6-mercaptopurine. - Mechanism: They disrupt the sequence of DNA by being incorporated instead of the normal nucleotide or irreversibly bind to the constituting enzyme and render it ineffective. - Side effects: nausea & vomiting, renal & liver dysfunction, diarrhea, hand-foot syndrom, conjunctivitis, cerebellar syndrom,
Anti tumor therapies • Vinca alkaloids (plant derived agents): - Examples: Vincristine, Vinblastine. - Mechanism: They bind to intracellular tubulin and inhibit microtubule formation which constitutes the spindle during mitosis. Thus mitosis is arrested at metaphase. - Side effects: nausea & vomiting, mucositis, peripheral neuropathy, neuropathy, alopecia.
Anti tumor therapies • Antimitotics antibiotics: - Examples: Adriamycin, actinomycin D, mitomycin C, bleomycin. - Mechanism: intercalation between opposing DNA strands leading to disrupted DNA function. Another mechanism involves the impairment of DNA & RNA synthesis and generation of toxic free radicals . - Side effects: nausea & vomiting, alopecia, flu-like, cardiomyopathy, pulmonary fibrosis, mucositis, discoloration & thickening of skin over joints.
Anti tumor therapies • Chemotherapy: • Resistance to chemotherapy: - Some anticancer drugs are effective as single agents (e.g., Cisplatin for treatment of testicular CA), but combination therapy with multiple drugs is common practice. The major advantage with combination chemotherapy is the increased chance to overcome drug resistance.
Anti tumor therapies • Chemotherapy: • Resistance to chemotherapy: - Drug resistance maybe inherent to tumor cells or may arise after exposure to anticancer drugs: * Pancreatic, renal, non-small cell lung CAs >>>>> poor responders to chemotherapy. * Breast, ovarian, small cell lung CAs, acute leukemias & lymphomas >>>>> high initial response rate but durable responses are rare bec of the acquisition of drug resistance mechanisms.