Download
1 / 41
420 likes | 952 Vues
Paracetamol intoxication (acetaminophen, N- acetyl- p- aminophenol, APAP, NAPA, 4-hydroxy-acetanilide ). Aidah Abu El Soud Alkaissi RN, PhD. Pharmacodynamics . Paracetamol reduces pain and fever

E N D
Paracetamol intoxication (acetaminophen, N-acetyl- p-aminophenol, APAP, NAPA, 4-hydroxy-acetanilide) Aidah Abu El Soud Alkaissi RN, PhD Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Pharmacodynamics • Paracetamol reduces pain and fever • The mechanism of effect is prevention of synthesis of prostaglandine through inhibition of enzyme cyclooxygenesis in the central neural system • Dosage:Adults - 2 tablets up to 4 times a day, as needed. Do not take more than every 4 hours or exceed 8 tablets (4 doses) within 24 hours Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Pharmacokinetics • Absorption • After oral application, Acetaminophen is rapidly absorbed from the stomach and small intestine • Plasma concentration reaches its peak after 15 to 60 minutes after taking, a life half time in plasma is 1 to 4 hours after the therapy dose • Extraction • 98% of Paracetamol is extracted through kidneys as conjugants Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Paracetamol intoxicationAcetaminophen (N-acetyl-p-aminophenol)Pathophysiology • Is one of the most common pharmaceuticals associated with both intentional and accidental poisoning • Biochemical evidence of maximal damage may not be attained until 72-96 hours after ingestion of the overdose Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
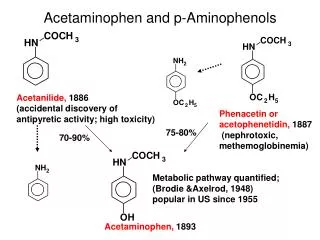
Paracetamol intoxicationAcetaminophen (N-acetyl-p-aminophenol) • Acetaminophen is primarily biotransformed to nontoxic products in the liver via conjugation with glucuronic acid and, to a lesser degree, sulfate, and eliminated by the kidneys • A small proportion (5-15%) of acetaminophen is metabolized through the cytochrome P-450 enzyme pathway producing a highly reactive and toxic metabolite, N-acetyl-para-benzoquinoneimine (NAPQI) which may cause hepatic injury Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Paracetamol intoxicationAcetaminophen (N-acetyl-p-aminophenol) • The hepatic glutathione conjugates the NAPQI to produce N-acetyl-p-aminophenol (APAP) mercapturate and APAP-cysteine which are both nontoxic metabolites • Acetaminophen exposure becomes toxic when glucuronidation and sulfation pathways become saturated and cellular glutathione stores are depleted • In such cases, NAPQI binds to cellular proteins and membranes, causes disruption of protein function and damage to cell membranes, and leads to cell injury and death, causing centrilobular hepatic necrosis Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Paracetamol intoxicationAcetaminophen (N-acetyl-p-aminophenol) • Defined as a peak plasma alanine aminotransferase (ALT) activity exceeding 1000 IU/L • Aspartate transaminase (AST) exceeding 1000 IU/L indicates severe liver damage • At risk of severe liver damage if he/she has ingested more than 150mg paracetamol/kg body weight, or, in adults, more than 12g (24 standard tablets) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Paracetamol intoxicationAcetaminophen (N-acetyl-p-aminophenol) • Without specific antidotal therapy, 10% would suffer severe liver damage but 1 to 2% will develop fulminant hepatic failure and this is often fatal • One to 2% of patients develop acute renal failure requiring dialysis Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Frequency • In the US: Acetaminophen is one of the most common pharmaceutical agents involved in overdose, as reported to the American Association of Poison Control Centers • APAP toxicity is the most common cause of hepatic failure requiring liver transplantation in Great Britain and the second most common cause of liver failure requiring transplantation in the United States Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Clinical Assessment Amount of Ingestion • The time of ingestion is essential for determining whether antidotal therapy is required immediately • Clinicians should also consider the possibility of co-ingestion of other agents Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Diagnosis • blood for urgent estimation of the plasma paracetamol concentration after 4 hours since the time of ingestion • Blood and urine toxicologic screens & a pregnancy test if the patient is a menstruating female • Assess whether the patient is at enhanced risk of severe liver damage Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Enhanced Risk of Severe Liver Damage • Consume alcohol • Malnourished • Take enzyme-inducing drugs (e.g. carbamazepine (Tegretol), Anticonvulsant, antimanic agent, Phenytoin, phenobarbitone, primidone, rifampicin • Those with conditions causing glutathione depletion (e.g. malnutrition, eating disorders and HIV infection) may be at risk of liver damage from lower plasma paracetamol concentrations than others Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Signs and symptoms • Consciousness is not depressed unless other drugs have also been taken or there is a very high plasma paracetamol concentration of the order of 6.62 mmol/l (1000 mg/l) with a metabolic acidosis • Nausea and vomiting usually develop within a few hours of ingestion of a hepatotoxic dose of paracetamol • Elevation of the plasma alanine and aspartate transaminase activity from normal values of less than 40 to as much as 10 000 or even 20 000 U/l caused by their release from a large mass of necrotic hepatocytes Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Signs and symptoms • With mild to moderate increases in the plasma bilirubin concentration and prothrombin time ratio • The prolongation of the prothrombin time reflects acute impairment of synthesis of the vitamin K-dependent clotting factors • There is little or no increase in the plasma alkaline phosphatase activity unless liver damage is severe or the patient is a chronic alcoholic Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Signs and symptoms • Oliguric renal failure may become apparent within 24 to 48 h after the overdose of paracetamol, associated with back pain, microscopic haematuria and proteinuria • Fulminant hepatic failure may develop in severely poisoned patients from the third to the sixth day • Characterized by deepening jaundice, encephalopathy, increased intracranial pressure, disordered haemostasis with disseminated intravascular coagulation and haemorrhage, hyperventilation, acidosis, hypoglycaemia and renal failure. The prognosis is very poor Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Initial Treatment of Acute Acetaminophen Ingestion • Acetaminophen levels greater than 150 µg/ml at four hours post ingestion or levels above the nomogram line should be considered toxic Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion I. Gastrointestinal Decontamination • When acetaminophen is the only substance ingested, gastric lavage or ipecac administration may be beneficial for large ingestions in patients who present within two hours of ingestion • Ipecac is contraindicated in the setting of altered mental status, or a co-ingestion that potentially can cause seizures or rapid deterioration of mental status Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestionI. Gastrointestinal Decontaminatio • Protracted vomiting induced by ipecac may cause difficulty with the subsequent administration of activated charcoal or acetaminophen antidot • Some toxicologists who feel that gastric lavage has not been proven to be helpful and should be used only if the ingestion is potentially rapidly fatal and the patient presents to the emergency department within 1 hour of the ingestion Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion II. Activated charcoal administration • Administration of 50g charcoal may be considered if: • more paracetamol than 150mg/kg body weight is thought to have been ingested • it can be given within one hour of the overdose • ingestion of unknown quantity • ingestion of 100mg/kg or more if known liver disease, anorexia, alcohol abuse, or on anticonvulsant or barbiturate therapy Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion II. Activated charcoal administration • Those that argue against giving charcoal believe that it may decrease the bioavailability of the antidote N-acetylcysteine (NAC) • The proponents of giving activated charcoal recommend increasing the initial loading dose of NAC (140 mg/kg) by 30-40% Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion II. Activated charcoal administration • Repeat doses of activated charcoal have no significant effect on acetaminophen ingestion because of its rapid absorption and limited enterohepatic excretion • Use of cathartic agents (such as sorbitol, magnesium citrate, or magnesium sulfate) is common but probably does not affect acetaminophen absorption Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion III. Antidote Therapy for Acetaminophen ToxicityN-acetylcysteine (NAC) • Is the N-acetyl derivative of the protein amino acid L-cysteine • NAC is available as a nutritional supplement and as a drug • It is given orally or by slow intravenous infusion in the treatment of acetaminophen overdose. NAC is theorized to work through a number of protective mechanisms • Early administration of NAC, within 8 hours of ingestion, is nearly 100% hepatoprotective Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion III. Antidote Therapy for Acetaminophen ToxicityN-acetylcysteine (NAC) • NAC is also used in the treatment of respiratory disorders, such as acute and chronic bronchitis associated with the production of excessive or viscous mucus • For such respiratory disorders, it is delivered as an inhalant Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestionIII. Antidote Therapy for Acetaminophen ToxicityN acetylcysteine (NAC • NAC is a glutathione precursor that repletes glutathione storage • N-acetylcysteine may reduce the severity of liver necrosis by directly conjugating with and/or reducing the reactive metabolite NAPQI (Tee et al 1986) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestionIII. Antidote Therapy for Acetaminophen ToxicityN acetylcysteine (NAC • NAC also functions as an anti-inflammatory and antioxidant and has positive inotropic effects • NAC increases local nitric oxide concentrations, and this vasodilatory effect on microcirculatory blood flow enhances local oxygen delivery to peripheral tissues • These vasodilating effects decrease morbidity and mortality even in the setting of established hepatotoxicity Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Efficacy of NAC • Results of the Multi-center Oral N-Acetylcysteine trial suggest that NAC is beneficial up to 24 hours after ingestion • Other studies comparing a 48-hour oral protocol in the United States vs. a 20-hour intravenous NAC protocol in Britain found that both modalities were effective if started within 8-10 hours of ingestion • A 72-hour oral NAC protocol appeared to be more effective for high-risk patients presenting late (i.e., 16-24 hours following ingestion) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Efficacy of NAC • Prior to the advent of an antidote, the mortality rate of patients at probable risk of hepatotoxicity (> 200 µg/ml at four hours) was reported between 5.3% and 24% • The overall mortality rates reported with the 20-hour intravenous NAC protocol and the 72-hour oral protocol were 2% and 0.68%, respectively • No fatalities were reported in any protocol in which NAC therapy was instituted within 10 hours of ingestion Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Mechanism of Action of N-acetylcysteine • The antidote NAC is available in the United States as an oral form • An intravenous form is available in Canada and Europe but is not yet FDA approved in the USA • Start treatment with NAC in patients whose plasma paracetamol concentration related to the time from ingestion is above the relevant line on the graph (Nomogram) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Nomogram For Paracetamol Poisoning. Check you are using the correct units micromols/LitreA level of over 1300 at 4 hours requires treatment (1000 for high risk patients) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Timing of NAC Administration • The optimal time is within the first eight hours following acetaminophen ingestion • During this period and regardless of the amount ingested and the acetaminophen level, NAC is uniformly effective • After the eight-hour post-ingestion period, the efficacy of NAC decreases progressively Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Timing of NAC Administration • If a patient with acetaminophen overdose presents more than eight hours after ingestion; • an acetaminophen level should be sent to the lab, • NAC should be started immediately for those with suspected significant ingestions while awaiting the result • decisions regarding whether NAC therapy should be continued or discontinued depend on the result of the acetaminophen level Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
PO administration of NAC - ADULT • 140 mg/kg loading dose, • followed by 70 mg/kg q4h for 17 additional doses (total 1330 mg/kg over 72 h) Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Dosage for NAC infusion - ADULT • (1) 150mg/kg IV infusion in 200mL 5% dextrose over 15 minutes, then • (2) 50mg/kg IV infusion in 500mL 5% dextrose over 4 hours, then • (3) 100mg/kg IV infusion in 1000mL 5% dextrose over 16 hours Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Adverse reactions to NAC and their management • Adverse effects which may be localised to the area surrounding the infusion site or may be more generalised • These usually occur during the first 30 minutes of administration when large amounts of NAC are being given rapidly • They include nausea, flushing, itching, erythematous rash, urticaria, angioedema, bronchospasm and, rarely, hypotension or hypertension Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Delayed NAC Therapy • Recently, a randomized blinded trial from Britain evaluated the efficacy of late NAC therapy in patients with fulminant liver failure and Grade III or IV hepatic encephalopathy • The investigators demonstrated significant improvement in survival rate (48% vs 20%) with NAC therapy and decreased incidence of elevated intracranial pressure and systemic hypotension Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Delayed NAC Therapy • In another study examining effects of NAC on the microcirculation of different organs in patients with either Grade III or IV hepatic coma and fulminant liver failure from different etiologies, the authors discovered that NAC increased cardiac index, decreased vascular resistance, and improved oxygen delivery and extraction • This evidence supports NAC therapy for acetaminophen-toxic patients regardless of the time of ingestion, the optimal dose and duration of late NAC therapy remains undefined Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Hepatic Necrosis Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Hepatic Necrosis Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion V. Liver Transplant • Admit patients to an ICU setting if they show signs of significant hepatotoxicity; hepatic failure; or other potentially life-threatening, coexisting, toxicologic, or medical issues • Liver transplantation may be the last viable option in patients with fulminant hepatic failure from acetaminophen • The shortcomings of this practice include deciding the optimal timing for referral and the relatively limited experience with liver transplantations for acetaminophen hepatic damage Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Management of acetaminophen ingestion V. Liver Transplant • In a study examining liver transplant for patients with fulminant hepatic failure, advanced hepatic coma, severe acidosis, markedly prolonged prothrombin time, and evidence of significant renal failure • four of six patients undergoing liver transplantation survived for one year, whereas only four of 23 patients with the same clinical indications but who did not receive liver transplantation survived for the same period of time Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing
Thank You Dr. Aidah Abu El Soud Alkaissi An-Najah National University Faculty of Nursing