Download
1 / 16
170 likes | 200 Vues
Learn about acetaminophen overdose, its toxic effects, metabolism, factors affecting toxicity, and clinical presentation. Discover the management steps, including N-acetylcysteine administration and laboratory analysis.

E N D
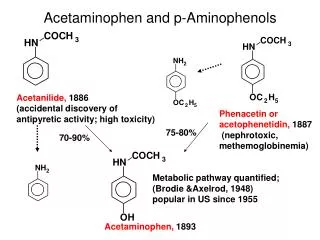
Acetaminophen N-acetyl-P-aminophenol (APAP)
Paracetamol Overdose -Most common drug taken in overdose -As little as 12g can be fatal (therapeutic dose = 2.6 gm/24 hour) -It is a hepatic and renal toxin (Centrolobular necrosis) -More toxic if liver enzymes are induced or with reduced ability to conjugate toxin (alcoholics, phenytoin, phenobarbitone) -The safety of acetaminophen depends on the availability of electron donors such as reduced glutathione (GSH) and other thiol-containing substances required to detoxify NAPQI.
Met pathways of APAP 1- Hepatic glucuronide conjugation(40-65%) Hepatic sulfat conjugation(20 - 45%) 90% inactive metabolites excreted in the urine. 2- Excretion of unchanged APAP in the urine (5%). 3- Oxidation by P450 cytochromes to NAPQI(5-15%) GSH combines with NAPQI nontoxic cysteine/mercaptate conjugates excreted in urine. Hepatic glucuronide conjugation(40-65%) Hepatic sulfat conjugation(20 - 45%)
Mechanism of Toxicity: The ingested APAP undergo oxidative metabolism by CYP- 450 to reactive intermediate metabolite(N-acetyl –P-benzoquinone imine=NAPQI) which is rapidly bounded to glutathion ,detoxified through conjugation pathway ,and excreted. In the presence of adequate GSH stores , there is no fear from any toxicity. However, overdose of APAP saturate the conjugation pathways and NAPQI overwhelms the GSH detoxifi-cation mechanism , finally leading to liver necrosis and may be death.
What happens to APAP metabolism in an OD situation? 1-Saturation of glucuronidation and sulfation pathways 2-Amount of APAP metabolized by p450 cytochromes to NAPQIincreases. 3-Normally NAPQI is detoxified by reduced GSH (glutathione) and thiol containing substances. 4-In OD: rate and quantity of NAPQI formation overwhelms GSH supply and regeneration: elimination of NAPQI prolonged free NAPQI binds critical intracellular proteins with sulfhydryl groups cellular dysfunction and cell death.
Factors which adversely affect APAP metabolism 1-Upregulation (i.e. induction) of CYP 2E1 enzyme activity: smoking, barbituates, rifampin, carbamazepine, phenytoin, ethanol 2-Decreased glutathione stores (malnutrition) 3-Frequent dosing interval of APAP. 4-Prolonged duration of excessive dosing.
Glutathione stores are determined by: -Age -Diet -Liver disease -Fasting prior ingestion -Chronic malnutrition -Anorexia -Gastroenteritis -Chronic alcoholism -HIV Glutathione replacement by sulfhydryl compounds: -Eating -NAC GSH stores
Renal toxicity Organ dysfunction results everywhere where local oxidative metabolism (via p450) creates NAPQI that cannot be detoxified direct toxicity: cytochrome P-450 enzymes produce NAPQI in the renal tubules NAPQI binds cellular macromolecules acute tubular necrosis. (25% of hepatotoxic cases) Hepatorenal Syndrome &Volume depletion
Other organs damaged Heart myocarditis Pancreas pancreatitis It is controversial whether these entities are part of multisystem organ failure (MSOF) from fulminant hepatic failure (FHF) or from the local accumulation of toxic metabolites.
Clinical presentation Phase 1(few hrs after ingestion up to 24 hr) :Malaise , nausea , vomiting and diaphoresis. Phase 2 (24-72 hrs after ingestion) : Increase in liver enzymes, serum bilirubin , prothrombin time , and pain in the right upper abdominal quadrant. Phase 3 (72-96 hrs after ingestion) : Peak in the liver function, altered consciousness, hypoglycemia, jaundice , and coagulation abnormalities. Hepatic failure can develops in 4th or in the 5th day if hepatic damage is sever. Myocardial necrosis, pancreatitis , heamolytic anemia and skin rashes may develop but are rare. Phase 4 (7-10 days after ingestion) : Liver enzymes abnormalities reaching resolution. If hepatic damage is massively sever sepsis and death may occure at 7-10 days
Laboratory analysis 1-Determination of plasma APAP level. 2-Monitoring liver profile including serum ALT, AST , bilirubin , glucose , prothrombin time, platelet count…etc 3- Determination of kideny functions by measuring plasma creatinine and BUN. 4-ECG for assessment of myocardial injury. 5- Urine analysis.
Management Steps: General measures (if the patient is presented to ER within 4 hrs of ingestion -Gastric lavage -Activated charcoal ,cathartics (saline sulfate are prefered to enhance sulfate metabolic pathway). glucose, bicarbonate, Vit K for elevated prothrombin time <8 hours -Take level of APAP after four hours (Peak concentration at 4 hrs then hepatic metabolism) -Start N-aceylcysteine (antidote) if APAP concentrationis high =APAPis on or above nomogram tx line. -Patients should be advised to return to hospital if vomiting or abdominal pain develop or reoccur.
Management 2 >8 hours Urgent action required because the efficacy of NAC declines progressively from 8 hours after the overdose Therefore, if > 150mg/kg or > 12g (whichever is the smaller) has been ingested, start NAC immediately, without waiting for the result of the plasma paracetamol concentration >24 hours Still benefit from starting NAC
N-acetylcysteine (Antidote) Supplies glutathione precursor (cysteine) Dosage for NAC infusion (1) 150mg/kg IV infusion in 200ml 5% dextrose over 15 minutes, then (2) 50mg/kg IV infusion in 500ml 5% dextrose over 4 hours, then (3) 100mg/kg IV infusion in 1000ml 5% dextrose over 16 hours Side-effects Flushing, hypotension, wheezing, anaphylactoid reaction -Alternative is methionine PO , it increase GSH synthesis. -Hemodialysis and hemoperfusion can be considered in extremly elevated APAP level.