Download
1 / 30
300 likes | 326 Vues
Learn about Health Savings Accounts, Consumer Directed Health Care, and Consumer Directed Health Plans. Discover funding mechanisms, roles, dynamics, and tools to make informed healthcare decisions.

E N D
HSA-CDHC-CDHPHealth Tech Net Rod Moyer & Jeff Hogan rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
What Is This Stuff • HSA – Health Savings Account • CDHC – Consumer Directed Health Care • CDHP – Consumer Directed Health Plan • Currently these terms are also in use as imprecise buzzwords, especially in the press rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
A CDHP Should Consist of: • A high deductible coverage of some sort • One or more funding mechanisms for the costs of care below the deductible • Tools for the consumer to use to make care decisions rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Funding Mechanisms • Health Savings Account (HSA) – The “new” mechanism from Medicare Reform Act • Health Reimbursement Arrangements (HRA) – Defined by IRS a few years ago • Flexible Spending Accounts (FSA) – Around for a long time, also referred to as Sec. 125 programs rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Why Mention All Three? • Many CDHPs utilize more than one of these • Each is defined via IRS requirements • The requirements are different for each and in some cases there are rules about how they interact rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
For Example, Funding Source & Balances • For FSAs, the funds are the employees funds from a payroll deduction, and any year-end balance is lost. • For HRAs, the funds are purely from the employer and any balance can be rolled if the employer chooses. • For HSAs, anyone can fund, and any balance belongs to the employee. rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Or Funding Cycle • FSA is funded with payroll deduction—usually bi-weekly or monthly, however entire balance is available on day one • HRA may be funded in periods defined by employer—could be annual, monthly, quarterly, but only the amount paid in is available rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
HSA Funding Cycle • The money can be put into the HSA at any time up to April 15 of the following year, HOWEVER: • The maximum balance is 1/12 of the annual amount for each month of eligibility, • Expenses are only allowed to be paid after the HSA has been established • Many people will not have the full amount just sitting around rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
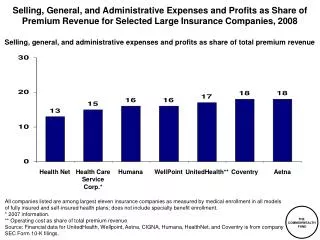
What Do CDHPs Try to Achieve? • Slow the rate of increase in healthcare & coverage costs • Increase the amount of cost sharing—or if you wish to be blunt, cost shifting • Turn healthcare “users” into healthcare “consumers” rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
All the Roles Change • Health plans • Employers • Agents/Brokers • Employees/Patients • Providers rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
The Patient Becomes a Consumer • PRICE/QUALITY TRANSPARENCY—CONSUMERS WILL HAVE TOOLS TO SEE WHAT THINGS COST, WHETHER THE PROVIDER/FACILITY ARE CAPABLE OF PERFORMING THE SERVICE AND WHAT “BEST PRACTICES” IS FOR THE PROCEDURE rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
What are the Dynamics? • The cost increases from the late ’90s through today parallel the high level of increases in the late ’80s that lit the fire under the shift to HMOs • 2005 increases are forecast to be between 7% and 11% which, while a somewhat lower rate, is still significant rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
How do you Transition Employees? • TAKE EMPLOYEES WHO ARE ACCUSTOMED TO USING COPAY PLANS AND GIVE THEM HIGH DEDUCTIBLE OPTIONS WITHOUT AFFECTATION. • OFFER FINANCIAL INCENTIVES, VIA CONTRIBUTION STRATEGIES TO ELECT INTO PLANS WITH HIGHER EXPOSURE. • FUND TAX FAVORED ACCOUNTS TO ENCOURAGE EMPLOYEES TO BE ARBITERS OF THEIR OWN RISK rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Transitioning • PROVIDE EXCELLENT EDUCATION TO EMPLOYEES TO TURN THEM INTO EDUCATED CONSUMERS OF HEALTHCARE WHO APPRECIATE THEIR BENEFITS PACKAGE • SELECT THE HEALTH PLAN THAT IS MOST INTEGRATED AND SEAMLESS AND PROVIDES THE BEST CDHP PACKAGE rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
The Strategy is Multi-year • There is a lot that is different/new • It’s really a culture change and that takes time • Strategy should be planned out over several years • Phase in incentives, constant education and training, capitalize on experience rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Tools & Technology • If CDHP approaches are expected to have impacts on the costs and the quality of healthcare, individual consumers must be able to act more effectively than the trained professionals who currently administer healthcare plans. • If individual consumers need to achieve better outcomes in terms of costs and treatment results they need tools and the training to use them. rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Tools for Making Cost Decisions • Consumers need access to both actual specific costs for specific procedures performed by specific providers in specific settings and information about ranges of costs and specific costs of alternatives to form a context in which alternatives can be evaluated. • These need to be real costs, not charges—the amount the health plan would pay. rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Data vs. Information • Note that for this element and all other elements, the need is for information not just data • Data must be taken, manipulated and arrayed in a way that allows for sorting and ranking and combining and re-combining elements to facilitate and support decisions rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Qualitative Information • In addition to, and perhaps more important than costs, information must be made available about qualitative aspects of care including: • Proximity • Outcomes—mortality, morbidity, complications and quality of life • Number of procedures performed • Relative status compared to others • Etc. rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Decision Algorithms • Cost and qualitative information have to be able to be combined within algorithms that allow consumers to “weight” elements and factors • Consumers should be able to adjust the factors to refine their thinking • The results should be arrayed in a comparative fashion rather than an absolute answer rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Benefit Selection Information • Consumers faced with choices about healthcare coverage selections as well as about appropriate account funding decisions where no benefit choice exists should be provided with information about the costs and implications of alternatives • Algorithms should be provided that permit consumers to plug in personal information rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Fund Management & Tracking • Each consumer could have an FSA, an HRA and an HSA depending on benefit design • Consumers can and eventually will have multiple HSAs in much the same way they have multiple IRAs • The rules for each type of fund and how they may be expended are different rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Fund Management & Tracking • The current balances for each type of account will be different both on the basis of how they are funded and expenses posted • The account information must be real time to avoid decisions made in error • The accounting must be banking type accounting in terms of accuracy and transaction documentation rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Fund Management & Tracking • While transactions need to be documented and supported in a banking manner, the accounts themselves will necessarily be adjusted with typical claims-type adjustments • The funds must be able to handle “split” transactions where part is under the deductible and part is insured rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
EFT • EFT may or not be a component of the funds • If EFT is a component real time balances, near real time adjudication and split transactions should be supported • If EFT is NOT a component, consumers will be required to “float” funds to at least some providers and claim reimbursement rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
EFT • Consumers may need to pay providers thousands of dollars from funds that have not yet built up those balances with or without EFT • Consumers may need to determine the balances of their various accounts from home, work and while at provider sites with or without EFT rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Additional Features • A well developed CDHP will also provide many of the following: • Onsite or transparent access to clinical fact finders & algorithms • Onsite or transparent access to a full “drug finder” solution built on the specific benefits and formulary of the consumer • Telephone access to all the same information • Knowledgeable and specifically trained CSRs rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Additional Features • Employer access to “Help” and algorithm features to assist employees • On line enrollment, disenrollment and benefit changes • Hard copy flow sheets to mirror online algorithms • Enhanced reporting to support performance analysis rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Additional Features Enhanced security for web portals Enhanced security for EFT including PINs and possibly biometrics to protect funds EFT transaction “lockouts” to prevent erroneous EFT transactions for expenses that are non-Sec. 213 rodmoyer@ix.netcom.com jhogan@rogersbenefit.com
Rod Moyer rodmoyer@ix.netcom.com Ph-215-345-5729 One Dartmouth Court Doylestown, PA 18901 Jeffrey J. Hogan Regional Manager Rogers Benefit Group jhogan@rogersbenefit.com Ph-860-677-6696 1 Forest Park Drive Farmington, CT 06032 Thank You rodmoyer@ix.netcom.com jhogan@rogersbenefit.com