Download
1 / 71
710 likes | 926 Vues
Self-Sufficiency In Solid Organ Transplantation: How Does Canada Stack Up?. John S. Gill, M.D., M.S. Associate Professor Of Medicine Michael Smith Scholar University of British Columbia St. Paul’s Hospital Vancouver, Canada jgill@providencehealth.bc.ca

E N D
Self-Sufficiency In Solid Organ Transplantation:How Does Canada Stack Up? John S. Gill, M.D., M.S. Associate Professor Of Medicine Michael Smith Scholar University of British Columbia St. Paul’s Hospital Vancouver, Canada jgill@providencehealth.bc.ca Edmonton ( Where the streets have no name) June 23, 2010
Disclosures Disclosures – NONE
“Self-Sufficiency in Transplantation” • World Health Organization “Equitably meeting the transplantation needs of a given population using resources from within that population”
Presentation Goals • Discuss key determinants of self –sufficiency (focus on kidney transplantation) • Provide Canadian Data and International Comparisons • Discuss how Canada might improve
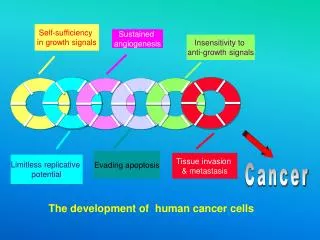
Self-sufficiency: Determinants1. Incidence of End Organ Failure
International Comparisons of ESRD • US Overall: 350 per million • US Blacks: 530 per million • US Asians: 205 per million • US Whites: 210 per million • Canada: 156 per million USRDS 2007 ADR
Treated ESRD vs. “Real” ESRD • Rate of ESRD treatment is dependent on • Surviving competing risk of death • Being offered renal replacement therapy • Accepting renal replacement therapy
CKD Prevalence in Norway vs. United States Hallan et al JASN 17:2275-84; 2006
Timing of Nephrology Contact and Progression to ESRD in British ColumbiaLevin et al AJKD 2008
Incidence of End Stage Disease • After accounting for differences in ethnicity prevalence of CKD is relatively similar in different countries • Progression to ESRD is markedly different between countries • Canada is probably doing a lot better than the United States but not as well as some European nations
Conversion Rate of Potential Donors(<61 yrs and Ventilated)2005-8
Number of Organ Transplanted Per DonorCanada 2007 U.S: 2.99 organs transplanted per donor Transplant Collaborative Goal = 3.75
Proportion of Deceased Donors where both kidneys transplanted 2000 U.S: 74% of all kidneys transplanted (94% SCDs, 56% of ECD transplanted)
Discard of Deceased Donor Kidneys 2000-3Cecka et al Transplantation 2006 81;966-71
Organ Utilization Securing more donors but non-transplantation of organs is an issue in the United States Canada’s transplantation rate is probably higher than that in U.S. but lower than E.U.
Self-sufficiency: Determinants4. Organ Allocation • Implement equitable allocation schemes that optimize utility from available organ supply
Background Merion et al. (JAMA 2005) recommended ECD kidneys be allocated to transplant candidates: Aged 40 or older with diabetes Aged 40 or older with wait-time >1350 days These evidence based recommendations are not mandated in the US
Purpose To determine the utilization of ECD kidneys according to evidence based recommendations over time To quantify the consequences of non-recommended utilization of these organs
Non-recommended ECD use decreased over time in young patients, but increased for older, non-diabetic patients with short wait-times
Patients under 40 who received an ECD kidney spent an extra 9 months on dialysis after allograft failure compared to those that received an SCD kidney PATIENTS < 40 YEARS OF AGE SCD ECD Patient survival Patient survival ∆ AUC= 10 months ∆ AUC= 19 months Death censored Graft survival Probability of Remaining Event Free Death censored Graft survival Time from Transplantation (years) Time from Transplantation (years) SCD recipients returned to dialysis after allograft failure for an average of 10 months ECD recipients returned to dialysis after allograft failure for an average of 19 months
Patients aged 40-59 who received an ECD kidney spent an extra 6 months on dialysis after allograft failure compared to those that received an SCD kidney PATIENTS AGED 40-59 YEARS WITH NO DIABETES AND WAIT-TIME<1350 DAYS SCD ECD Patient survival ∆ AUC= 5 months Patient survival Probability of Remaining Event Free Death censored Graft survival ∆ AUC= 11 months Death censored Graft survival SCD recipients returned to dialysis after allograft failure for an average of 5 months ECD recipients returned to dialysis after allograft failure for an average of 11 months Time from Transplantation (years) Time from Transplantation (years)
Summary Between 2006-08, ECD kidneys were allocated to nearly 25% of patients not recommended to receive an ECD kidney, based on existing evidence ECD recipients under the age of 40 returned to dialysis after allograft failure for an average of 19 months compared to 10 months among SCD recipients of the same age Non-diabetic ECD recipients aged 40-59 with wait-times <1350 days returned to dialysis after allograft failure for an average of 11 months compared to 5 months among SCD recipients
Balancing Utility and EquityCanadian Approach We know if more “ideal” donors are allocated to “young” recipients utility will be increased To ensure this does not disadvantage “older” recipients the number of these “ideal” kidneys shunted to “young” recipients must be limited If the age cut point for an “young” donor is a priori linked to the supply “non-ideal” kidneys that are prioritized to the “older recipients” equity will be maintained Donor and Recipient Cut Offs are NOT fixed and will change overtime
Establish Utility Based Definitions:Use Age because it is understandable and easy to implement • Young recipient – a patient who outlives their allograft • Old recipient – a patient who does not outlive their allograft • Young donor – avoid an a priori age cut off, limit will be set by number of “older donor” kidneys • “Old donor” – does not provide adequate years of graft survival to a young recipient BUT does provide adequate graft years to an “old recipient”…..also cannot shorten the lifespan of older recipient
Data Set Canadian Organ Replacement Register First kidney only deceased donor transplants 1995-2005 End of follow-up: Nov. 2007 Total N = 6,219 Working N = 6,191 CORR –not validated for outcomes Graft failure dates Dialysis and repeat transplantation dates captured Death dates are not validated
MV Models of Patient and Allograft Survival Over a 10 year period using Canadian Data • Maximum patient or graft survival = 120 months • Difference between Patient Survival Curve and Death Censored Graft survival curve = TIME BACK ON DIALYSIS AFTER Transplant Failure
“Young Recipient” < 55 years “Old Recipient” ≥ 55 years “Old donor” ≥ 55 years BUT: Donors ≥ 55 do not provide adequate years of kidney function to recipients 55-59 years Donor ≥ 55 do provide adequate function to recipients ≥ 60 years Observations
Supply and Demand:Young Donor age cut off determined by supply of “old donors” > 55years • Old donors >= 55 n = 461, these will be allocated to recips >60 • Young donor - upper age limit set by the supply of old donors = < 40 these kidneys would be allocated to recipients < 55 years • Recipients 55-59 would not be prioritized for Young or Old Donor kidneys – what impact would this have?
YD age 40 and allocated to <55 and “old donor” 55+ allocated to recips 60+ Actual allocation 2003-5 If allocation in place N=91 863 240 455 N=91 863 240 455
Deceased Donor Kidney Graft SurvivalFirst Transplant Unadjusted Data Sources USRDS, CORR