Download
1 / 37
370 likes | 506 Vues
Operating Efficiency and Safety in Minimal Access Surgery. Alfred Cuschieri Institute for Medical Science and Technology, Dundee Scuola Superiore Sant’Anna di Studi Universitari, Pisa. Operating Room Efficiency and Safety. Governance Teamwork Communication

E N D
Operating Efficiency and Safety in Minimal Access Surgery Alfred Cuschieri Institute for Medical Science and Technology, Dundee Scuola Superiore Sant’Anna di Studi Universitari, Pisa
Operating Room Efficiency and Safety • Governance • Teamwork • Communication • Standard operating procedures (SOPs) • Operational system • OR Design • Time and motion analysis • Stress • End of procedure scoring
Surgical Team Skills Based on CRM Model • System does not reduce authority/ accountability of Chief – remains in charge • Chief encourages all team members to contribute their knowledge and skills towards safe and effective execution of intervention • Components of good team dynamics:briefingsstandard operating procedures (SOP)check listsenvironment that encourages constant team interaction
Empower junior staff to voice their concerns Train senior staff to listen to perspectives of the rest of the team: honest concern or need for clarification NOT insubordination/ doubts about leaders’ ability
Standard Operating Procedures and Check Lists in Surgery • SOPs in surgery are the best practice guide lines based on evidence-based research • Still permit individual technique but ensure that critical steps are executed in a way that is documented to yield the best outcome • Check lists ensure that everything that needs to be done, actually gets done. Not ‘cookbook surgery’
Operational System Real time workflow processPatient and staff tracking system (RF identification tags)Clinical decision support systemAsset managementMeasuring outcomes OR architectureDesign considerations to maximize work flowDifferent interventional approaches require specific configuration/ layouts/ technologiesOperating room cluster to replace ‘all purpose OR’ Operational System vs. OR architecture
Communication and Technology within the OR • Common ground theory of team communication (Clark and Schaefer 1989, Clark 1996) • Common ground: efficiency depends on the individual’s working knowledge and/or assumptions about what other individuals within a communication setting (team) know • Communication success is reflected by the lowest level of shared knowledge (common denominator) • Established common ground (team knows all there is to know) results in more efficient communication (less time/ fewer words) and more successful outcome ( better task performance by team)
Caroline G.L. Cao , and Holly Taylor.Effects of New Technology on the Operating Room Team inWork with Computing Systems 2004. H.M. Khalid, M.G. Helander, A.W. Yeo (Eds) • Time motion and communication study: remote master-slave surgical robot (LaproTek) vs direct lap surgery Information need by the surgeon in order to complete operation without robot
Caroline G.L. Cao , and Holly Taylor.Effects of New Technology on the Operating Room Team inWork with Computing Systems 2004. H.M. Khalid, M.G. Helander, A.W. Yeo (Eds) • Time motion and communication study: remote master-slave surgical robot (LaproTek) vs direct lap surgery Information need by the surgeon in order to complete operation with robot
Nature of Motion Analysis • MA involves the study of patterns of movement • It draws conclusions on their efficiency based on comparisons made between certain recorded angles and paths of movement • Investigative technologies include:cinematography and video recordingoptoelectronic systemsgoniometerssystems combining photocells, light beams and timersNewer video software tracking system (Dundee) • Industrial MA is driven by need for information on:enhanced productivity (profit)improved quality
Motion Analysis & Telemetric EMG for research in grip forces, muscle recruitment and fatigue
Motion Analysis in Minimal Access Surgery • Investigation of ergonomic flow in the OR • Evaluation of proficiency in execution of operations in the OR • Study of joint movements and muscle recruitment and work – coupled with telemetric EMG • Research and development of instrumenation/ devices for laparoscopic surgery • Investigation of muscle fatigue and the overuse syndrome in MAS • Training of residents in skills laboratories • Motion analysis of the abdominal wall during insufflation
Benefits of Time-motion Analysis in MAS • Identifying unproductive and unnecessary activity during the surgical procedure itself • Improving OR layout and equipment design • Achieving better pre- and peroperative planning
Dundee StudyTime-Motion Studies During Laparoscopic Surgery Theatre Time • Anaesthesia induction • Surgical preparation • Set-up • Operative • Recovery • Instruments cleaning
Results • Activity of the scrub nurse • Time spent:Preparing instruments 23%Handing instruments 04%Following the procedure on the monitor 21%______________________________________ • Total 48% • Frequency of preparing and handing instruments 8 (21) 33 (14)
Disruption in the OR: Motion Analysis Study • Surgical workflow: Uninterrupted continuation of a surgical process within a specific observation period • Incidence of disruptive events: 114 episodes /hintra-operative conversations: 71/h - 1% delayinstrument change: 41/h – 33% delaySurgeon position change: 2/h – 44% delayNurse duty shift: 1/h - 12% delay Phone/ Page: 3/h – 3% delayExtraneous: 2/h • Disruptive events caused 4.1min delay/case/h and corresponded to 6.5% of procedure time Zeng et al Surg Endosc 2008, 22: 2171-7
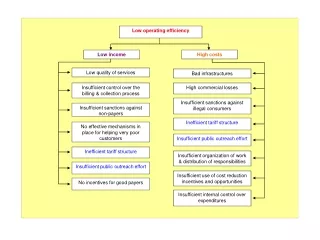
OR operational strategy • Assess demand and resource requirements • Plan for OR expansion • Continued professional development of Staff Surgical Service Strategic Development • Restructure governance mechanisms • Identify operational management requirements • Develop measurement and monitoring systems • Communication OR Governance , Policy & Management • Identify anaesthesia resource options • Restructure anaesthesia relationships • Team work based on CRM Anaesthesia and Staffing Needs • Reduce OR turnover time • Increase OR utilization • Increase available block time • Maximize staffing resources OR Operational Performance Improvement • Product standardization • Inventory reduction • Value analysis programs • Aged receivables management OR Supply Chain and Management
Apgar Neonatal Score • The Apgar score was devised in 1952 by Dr Viginia Apgar (anaesthetist) as a reproducible method of assessment of the health of newborn babies • The Apgar score is determined by evaluation based on five criteria (on a scale from zero to 2): Appearance, Pulse, Grimace, Activity, Respiration) then summing up the five values thus obtained • Max Apgar score (best condition) = 10 • Revolutionized neonatal care Apgar, Virginia (1953). A proposal for a new method of evaluation of the newborn infant. Curr. Res. Anesth. Analg.32 (4): 260–267
Surgical (Apgar) Outcomes Score A 10-Point Surgical Outcomes Score* 0 points 1 point 2 points 3 points 4 points Estimated blood loss (ml) > 1,000 601-1000 101- 600 ≤ 100 — Lowest mean arterial bp < 40 40 - 54 55 - 69 ≤ 70 — Lowest heart rate /min > 85 76 - 85 66 - 75 56 - 65 ≤ 55† Surgical score sum of the points for each category in the course of a procedure. †Occurrence of pathologic bradyarrhythmia, including sinus arrest, atrioventricular block or dissociation, junctional or ventricular escape rhythms, and asystole also receive 0 pts for lowest heart rate.
Thirty-day Outcomes for 767 Patients Undergoing General or Vascular Surgery, in Relation to Surgical Scores Surgical score Major complication/death Relative risk n % (95% CI) p Value* 0 - 2 4 3 75 20.6 (8.550.0) 0.0001 3 - 4 25 14 56 15.4 (7.233.1) 0.0001 5 - 6 123 20 6 4.5 (2.09.8) 0.0001 7 – 8 395 25 6 1.7 (0.83.8) 0.16 9 – 10 220 8 4 1 — c-statistic 0.72. *Chi-square test. Patients with scores of 9 or 10 served as the reference group
30-day mortality and major complications for 767 patients undergoing general or vascular surgery, in relation to surgical scores. *p 0.0001 for an association between surgical score and major complications/ death
Stress in Laparoscopic Surgery • Physical – morbidity • Mental – fatigue syndrome • Psychological – cardiac bio-signals of stressBeat-to-beat variability (MSSD) reflects changes in vagal activityPre-ejection period (PEP) beta adrenergic activityAverage heart rate (HRA) • Visual
Morbidity Involved • Nerve Injuries17 case reports of digital nerve injury (neuropraxia, axonotmesis • Back/ neck/ shoulder pain and arthralgia • Mental Stress • Surgical fatigue syndrome • Visual disturbances
Survey Lawther et al (2002 Surg Endosc) • Respondents50 surgeons • Morbidity reported:finger numbness (40%) unilateral (45%), bilateral (25%). Median duration 9 hours • Factors involvedmagnified operative viewdifficult dissection (tight grasp syndrome)lengthy procedures • Correlations reportedcase load – symptomatic group performed significanly more operations annuallyno correlation with years of practice
Body and Grip Stance of the Surgeon • Predominant stance of surgeon during laparoscopic surgery:static upright position with abducted arms • Same muscle groups are activated for long intervals of time • Position of surgeon does not alter • Magnified view exaggerates transmitted movements/ tremors – surgeons tend to grip instruments tighter than is needed to achieve fine instrument control
Operating From Images (Late Perception) • Interpretation:Image is first identified (snap shot) by saccadesImage is then scanned by slow-pursuit eye movements with fixation/ refixation by ocular muscles • Manipulation:Scans the picture and eye tracks the tips of the instruments • Display:NaturePosition and distance from surgeonImage quality
Effect of position of ‘image display’ on execution time Hanna et al p<0.0001 Rt = right, HL = level of hands, F = in front, EL = eye level, Lt = left
Effect of position of ‘image display’ ontask quality) Hanna et al p=0.08
Recognised Immediate Needs for a Modern OR • Integration of various technologies into physical layout of OR • OR design optimises work flow • Optimal OR size -70m2 (650feet2), flexible to support new technologies as they emerge • Clutter-free work space around patient and operating team • Ceiling mounted utilities • Integrated data and communication systems
Key Issues • Modern or future OR? • Generic or dedicated OR? • Single room OR or Interventional OR Cluster? • Increased safety in OR - technology vs. human factors? • Useful vs. status OR technologies ? • How do we assess OR functionality? • Consider patient and surgeon welfare • Time and motion and ergonomic studies needed to improve efficiency without compromise of safety • Safe operational systems – the players not just the theatre