Humidification
Humidification. Basic Concepts and Devices RT 31. Basic Concepts. Functions of the of the upper airway: assure that inspired gas is: Warmed (convection). Humidified via evaporation from the mucosa Filtered During exhalation: Expired gas transfers heat back to the mucosa (convection)

Humidification
E N D
Presentation Transcript
Humidification Basic Concepts and Devices RT 31
Basic Concepts • Functions of the of the upper airway: assure that inspired gas is: • Warmed (convection). • Humidified via evaporation from the mucosa • Filtered • During exhalation: • Expired gas transfers heat back to the mucosa (convection) • Condensation occurs on the mucosal surfaces and water is reabsorbed by mucus (rehydration)
Basic Concepts • As gas travels through the lungs it achieves BTPS: • Body temp ~ 37C • Barometric pressure • Saturation with water vapor (100% relative humidity @ 37C)
Basic Concepts • The point at which this occurs is called the isothermic saturation boundary (ISB) • Usually occurs ~ 5 cm below the carina • If the upper airway is bypassed or VE is significantly higher than norm, • The ISB will be deeper into the lungs and HUMIDITY therapy may be indicated
Basic Concepts • One of the most important, but least understood, aspects of pulmonary care is the role of humidity therapy. • Many care providers and most patients do not appreciate the role of hydration in liquefying secretions and facilitating the natural flow of mucus from the lower airways.
Basic Concepts • Pulmonary patients need: • adequate humidification of their inspired gases • controlled fluid balance • otherwise patients can become dehydrated. • Dehydration can make secretions more viscous and inhibit the mucociliary escalator activity of the airways, making secretions difficult to dislodge. • If these secretions block functional gas flow through the distal airways infections, atelectasis and other respiratory problems can easily occur.
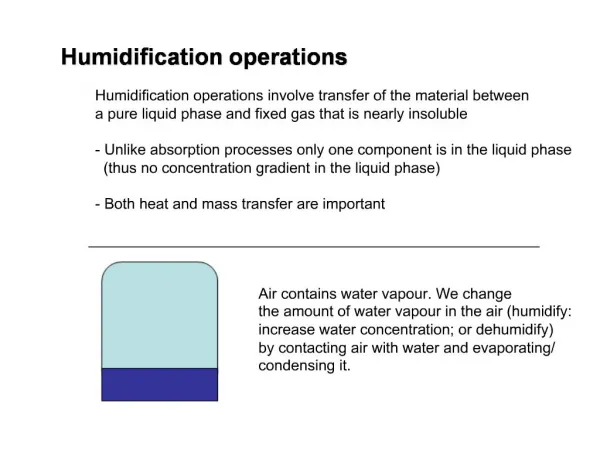
Basic Physical Principles of Humidity • Humidity is essentially the water vapor in a gas. • This water vapor can be described in several ways, as: • 1. Absolute humidity - The actual content of water vapor in a gas measured in milligrams per liter. • 2. Potential humidity - The maximum amount of water vapor that a gas can hold at a given temperature. • 3. Relative humidity - The amount of water vapor in a gas as compared to the maximum amount possible, expressed as a percentage • 4. Body humidity - The absolute humidity in a volume of gas saturated at body temperature of 37 C; equivalent to 43.8 mg/L
Formulas Used When Calculating Humidity • %RH=(absolute humidity/saturated capacity) x 100 • Refer to table 5-3 of Egan or 4-1 of Mosby. Calculations are based on temperature. See example on page 90 of Egan • %BH = (absolute humidity/43.8mg/L) x 100 • See example on page 97 of Egan • Absolute humidity: Refer to table 5-3 of Egan
Primary Humidity Deficit • If the atmosphere's relative humidity is less than 100%, the air of the atmosphere has what is referred to as a humidity deficit. • If outside air at 20°C has 14 mg/l of water vapor, and needs to have 17.3 mg/l to be fully saturated, it is said to have a primary humidity deficit of 3.3 mg/l. • 17.3 mg/L (potential) – 14 mg/L (absolute) = 3.3 mg/L (primary deficit) • Remember that the potential is based temp • The primary humidity deficit occurs in the atmosphere and represents the difference between what humidity there is and what there could be. • Primary Humidity Deficit = Potential Water Vapor Content - Actual Water Vapor Content
Secondary Humidity Deficit • This is the moisture deficit in the inspired air that the nose and upper airway need to compensate for. • The amount of water vapor the body needs to add to inspired air to achieve saturation at body temperature. • When air is breathed into the nasal cavity and heated to body temperature, its potential water vapor rises to 44 mg/l, which is the potential water vapor content of air at 37°C. • Therefore, unless the air of the atmosphere is at least 37°C and fully saturated, there exists a moisture deficit. • Secondary Humidity Deficit = 44 mg/l - Absolute Humidity.
How does a patient develop a humidity deficit? • Breathing a gas with little or no humidity and very high minute volume evaporation of the respiratory mucosa occurs • Bypass of upper airway: intubation, tracheostomy. • Dehydration due to illness, exposure, etc..... • Please understand Figure 4-3 of Mosby, page 94.
Water Losses • Insensible: skin and lungs • Sensible: urine, GI tract, sweat • Additive: vomiting, diarrhea, suction from intestines, severe burns, and fever • For each degree of temperature above 99F for over 24 hours, 1000m of fluid is required for replacement
Water Vapor Correction • Water vapor acts in most ways like any other gas, it creates a partial pressure when it’s in a mixture of gases. • That partial pressure depends • The amount of water vapor present • Which in turn depends on the temperature. • Unlike other gases in the air, changes in the barometric pressure of the atmosphere under normal conditions do not have much impact on the partial pressure of water.
Water Vapor Correction • As a result, it is best to calculate the partial pressures of the other gases in the air after the partial pressure of water vapor has been determined--especially when measuring the air within the lungs. • Inside the lungs, the partial pressure of water vapor is approximately 47 mm Hg. • This value is relatively constant because the air entering the lungs is normally saturated and at 37°C. • By subtracting the partial pressure of the water vapor from the total atmospheric pressure, you will find what is referred to as the dry gas pressure
Importance of Humidity • It is needed to maintain normal bronchial hygiene • It promotes functions of the normal mucociliary escalator • It maintains the body's vital homeostasis • Without humidity: • the nearly 100 ml of mucus secreted daily would become quite thick and tenacious. • actual lung parenchyma would dry up, causing a loss of normal compliance which would restrict lung movement and reduce ventilation.
Importance of Humidity If the upper airway were bypassed or dry gases were inhaled, a series of adverse reactions could occur, including: • Slowing of mucus movement • Inflammatory changes and possible necrosis of pulmonary epithelium • Retention of thick secretions and encrustation • Bacterial infiltration of mucosa (bronchitis) • Atelectasis • Pneumonia • Impairment of ciliary activity
Clinical Evaluation of the Need for Humidity and/or Aerosol Use • Patient's age and ability to move normal secretions • Neuromuscular status • Recent or planned surgeries • Trauma • Disease conditions • The presence of any of these may impair the patient's ability to cough and move secretions. • Another problem may occur when patients develop very thick and abundant amounts of secretions which cannot be moved with normal muscle activity--making humidity or aerosol therapy necessary.
Indications for delivery of humidified gases and aerosols • Primary indications for humidifying inspired gases include: • Administration of medical gases • Delivery of gas to the bypassed upper airway • Thick secretions in nonintubated patients
Indications for delivery of humidified gases and aerosols • Additional indications for warming inspired gases: • Hypothermia • Reactive airway response to cold inspired gas
Mucociliary Blanket • It’s natural escalator functions to clear airways via function of the ciliated mucosa. • This mechanism occurs from the larynx to the respiratory bronchioles. • Mucus is produced by goblet cells and submucosal glands. • Clara cells and tissue fluid transudation also contribute to airway secretions. • A wave-like motion of the cilia then move secretions upward toward the larynx where it is either swallowed or expectorated.
Sources of Mucus • Secretion from goblet cells and bronchial (mucous) glands. • The goblet cells, which are distributed throughout the epithelium of the mucosa, synthesize and secrete mucus into the airway.
Sources of Mucus • The mucous glands, which are in the submucosa, are the greater source of mucus. • Chronic irritation or disease can cause the number and size of goblet cells and mucous glands to increase, resulting in a larger and more viscous mucous blanket.
Effects of Mucous Layer • Ciliary activity, which moves the mucus, can be adversely affected if the mucous layer is changed. • A higher ratio of gel to sol layer will affect the flow of mucus by increasing cilia workload. • a decrease in the watery sol layer • or an increase in the viscous gel layer • The cilia are capable of continuing to beat even if the workload increases, but only to a certain level. • If the cilia become tangled in the thick mucus or are unable to penetrate the dense layer, the transport of the mucous blanket would stop, causing secretions to become retained in the respiratory tract.
Other factors that can impede ciliary activity and the flow of mucus include: • Tobacco smoke • Local environmental conditions • Pathology of the airway can impede clearance due to changes in the epithelium.
Sign/Symptoms of Inadequate Airway Humidification • Atelectasis • Dry, nonproductive cough • Increased airway resistance • Increased in incidence of infection • Increased work of breathing • Substernal pain • Thick, dehydrated secretions
Humidification Devices • The purpose of humidifiers is to deliver a gas with a maximum amount of water vapor content. • May be heated or unheated, and the factors affecting the efficiency of humidification devices include: • temperature • time of exposure between gas and water • surface area involved in the gas/water contact
Humidification Devices • As temperature rises, the force exerted by the water molecules increases, enabling their escape into the gas, adding to the humidity. • So the higher the tempthe more humidity • Longer exposure of a gas to the water increases the opportunity for the water molecules to evaporate during the humidifier's operation. • The greater the area of contact between water and gas, the more opportunity for evaporation to occur.
Humidification Devices • Space-efficient methods • Bubble diffusion • Aerosol • Wick technologies
Humidification Devices • Bubble diffusion: • Stream of gas is directed underwater • The gas is broken up into small bubbles • As gas bubbles rise, evaporation increases the water vapor content within the bubble
Humidification Devices • Aerosol: spraying water particles into gas • Aerosol (suspended water droplets) is generated in the gas stream • The greater the aerosol density (# of molecules), the greater the gas/water surface area available for evaporation
Humidification Devices • Wick: • Use porous water-absorbent materials to increase surface area • A wick draws water into its fine honeycombed structure by means of capillary action • The surfaces of the wick increase the area of contact between the water and gas
Blow-By • This “pass-over” type humidifier directs a dry gas source over a water surface area, and flowing it to the patient. • Because exposure area and time of contact is limited and it is not heated, this unit is not very efficient. • These units are often used in incubators and in certain ventilators, although many times the use of a heated element is added to improve this humidification system • Wick type or membrane type
Bubble Humidifier • Low-flow gas system • Provides flow lower than patient’s inspiratory needs. • Oxygen or air is humidified at 30%-50% relative humidity. • Gas is passed below the water’s surface in the form of bubbles. • Increase exposure time result in good humidification • Patient’s airway provide further humidification. • Should be used for NC use at 4lpm or above, but the higher the flow rate the less the exposure time. • Do not use with oximizers or venturi masks (these are common mistakes in the clinical setting)
Jet Humidifier • Forms aerosol • Baffle system to break up particles into smaller sizes • Bernoulli’s principle • Low flow • Large-volume jets are used for bland aerosol
Ultrasonic Nebulizers • Electrically powered • Uses piezoelectric crystal to generate aerosol • Transducer converts radio waves into high-frequency mechanical vibrations (sound) • These vibrations are transmitted to a liquid surface creating a geyser of aerosol droplets
Mist tents and hood • Kids don’t like things on their face • So tents and hoods are used to deliver bland aerosols • Sometimes referred to as croup tents • High flow rates should be used to prevent CO2 build up • Must use some kind of cooling device to prevent heat retention: refrigeration devices or even ice
Cascade Humidifier • High Flow: Provide vapor to entire gas flow • Used for mechanical ventilation, airway bypass (artificial airways) • 100% humidity • Usually heated to body temperature • Figure 4-7 of Mosby, page 99
Cascade Humidifier • Gas enters the cascade and travels to the bottom of the tower • Then it moves up through a sheet of plastic consisting of many tiny holes. • Tiny bubbles are produced and dissipate into water vapor, which are carried to the patient’s delivery circuit. • No back flow is allowed due to one-way valves • A heating element in the water reservoir heats the water to form warm gas. • Thermostat can be used to regulate and monitor temperature.
Heat and Moisture Exchangers (HME) or Artificial Noses • Functions similarly to the upper airway • Captures s exhaled heat and moisture and using it to heat and humidify inhaled gas. • Do not add heat or moisture--Use the body’s own heat and moisture. • Book statement: should be used short term, flow less than 10 lpm, and in the absence of thick secretions • Practical purposed: Used all the time! Changed every 24 hours.
Light weight Less dead space Reduce accumulation of condensation in tubing Decrease risk of infection (maybe) If moisture remains on filter for an extended period of time, airway resistance increases. Must be removed during aerosol therapy Dead space volume limits use for neonates and pediatrics. Heat and Moisture Exchangers (HME) or Artificial Noses
Aerosol Therapy Basic Concepts and Delivery Systems
Aerosol Therapy • It is important to remember that an aerosol is not the same as humidity. • Humidity is water in a gas in molecular form, while an aerosol is liquid or solid particles suspended in a gas. • Examples of aerosol particles can be seen everywhere: as pollen, spores, dust, smoke, smog, fog, mists, and viruses.
Aerosol Therapy • Aerosol therapy is designed to increase the water content delivered while delivering drugs to the pulmonary tree • Deposition location is of vital concern • Some factors that affect aerosol deposition are aerosol particle size and particle number.
Aerosol Output • The actual weight or mass of aerosol that is produced by nebulization. • Usually measured as mg/L/min also called aerosol density • Aerosol output does not predict aerosol delivery to desired site of action.
Particle Size • Heterodisperse: • aerosol with a wide range of particle sizes (medical aerosols) • Monodisperse: • aerosol consisting of particles similar in size (laboratory, industry)
Deposition • The aerosol particles are retained in the mucosa of the respiratory tract. They get stuck! • The site of deposition depends on size, shape, motion and physical characteristics of the AIRWAYS