Download
1 / 73
1.19k likes | 4.03k Vues
Hypotonia in Children. Dr. Mohamed Abunada Pediatric Neurology Department Dr. Al Rantisi Specialized Children Hospital. Definition. Muscle tone is defined as resistance to passive movement.

E N D
Hypotonia in Children Dr. Mohamed Abunada Pediatric Neurology Department Dr. Al Rantisi Specialized Children Hospital
Definition Muscle tone is defined as resistance to passive movement. Hypotonia means "low tone," and refers to a physiological state in which a muscle has decreased tone, or tension.
Hypotonia in Children • The maintenance of normal tone requires intact central and peripheral nervous systems. • Hypotonia is a common symptom of neurological dysfunction and occurs in diseases of the brain, spinal cord, nerves, and muscles . • One anterior horn cell and all the muscle fibers that it innervates compose a motor unit. The motor unit is the unit of force. Weakness is a symptom of all motor unit disorders. • A primary disorder of the anterior horn cell body is a neuronopathy, a primary disorder of the axon or its myelin covering is a neuropathy, and a primary disorder of the muscle fiber is a myopathy. In infancy and childhood, cerebral disorders far outnumber motor unit disorders.
Hypotonia in Children • Classification( Location) • Brain • Spinal cord • Peripheral nerves • Neuromuscular Transmission • Muscles • Systemic disorders
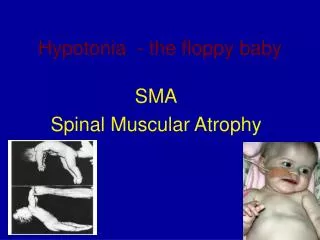
Hypotonia in Children Signs of Hypotonia • In supine, Frog position • Their heads lagwhen are held up • They slip throughat the shoulders • Do not stand upright on their legs • Form inverted Ushape in ventral suspension • Lie flatwhen in prone position.
Signs of Hypotonia • Poor ability to cough and clear airway secretions. • Poor swallowing ability • Crying character [weak, low pitched] • Paradoxical breathing pattern. Intercostal muscles paralyzed with intact diaphragm.
Signs of Hypotonia Ventral suspension Inverted U position The back hangs over the examiner's hand, and the limbs and head hang loosely Passive extension of the legs Pull to sit Head lag
Signs of Hypotonia The same infant in horizontal suspension. Note the inverted U posture.
Signs of Hypotonia A 12-week-old male infant with excessive head-lag evident on ‘pull-to-sit’. Note the hypotonic posture of the legs with external rotation.
Signs of Hypotonia Vertical suspension: The legs will be extended Decreased tone of the shoulder girdle allows the infant to slip through the examiner's hands
Approach to Diagnosis • The first step in diagnosis is to determine whether the disease location is in the brain, spine, or motor unit. • More than one site may be involved • The brain and the peripheral nerves are concomitantly involved in some lysosomal and mitochondrial disorders. • Brain and skeletal muscles are abnormal in infants with acid maltase deficiency and neonatal myotonic dystrophy. • Newborns with severe hypoxic-ischemic encephalopathy may have hypoxic injury to the spinal cord and the brain
Assessment Prenatal risk factors: • • History of drug or teratogen exposure • • Presence of polyhydramnios • • Maternal diseases (diabetes, epilepsy) • • Parental age • • Consanguinity • • Family history of neuromuscular disease • • Other affected siblings
History Taking • Any significant family history? • Was the Hypotonia present at birth? • Pregnancy and delivery history • Drug or teratogen exposure • Decreased fetal movements • Abnormal presentation • Polyhydramnios/ oligohydramnios • Apgar scores • Resuscitation requirements
Hypotonia in Children Clues in CEREBRAL Hypotonia Cerebral Hypotonia in newborns usually does not pose diagnostic difficulty. The history and physical examination identify the problem. • Normal or Brisk reflexes • Other abnormal brain functions: delay, seizures • Fisting • Movement through postural reflexes • Scissoring on vertical suspension • Dysmorphic features • Extra-cranial organ malformations
Hypotonia in Children Clues in MOTOR UNIT Hypotonia Disorders of the motor unit are not associated with malformations of other organs except for joint deformities and the mal development of bone structures. • Absent or Depressed reflexes • Intact brain function • Muscle atrophy • Fasciculations • Failure of movement through postural reflexes • No extra-cranial organ malformations
Classification HEAD - BRAIN • Hypoxic ischemic Encephalopathy • Hypotonic Cerebral Palsy • Benign Congenital Hypotonia • Excessive Subarachnoide space • Arthrogyroposis • Cerebellar disorders • Cortical Dysgenesis
Cerebral dysgenesis(Chronic Non progressive Encephalopathy) • may be due to known or unknown noxious environmental agents, chromosomal disorders, or genetic defects. • In the absence of an acute encephalopathy, hypotonia may be the only symptom at birth or during early infancy. • Hypotonia is usually worse at birth and improves with time. • Cerebral dysgenesis is suspected when hypotonia is associated with malformations in other organs or abnormalities in head size and shape. • Magnetic resonance imaging (MRI) of the head is advisable when cerebral malformation is suspected. • The identification of a cerebral malformation provides useful information not only for prognosis, but also on the feasibility of aggressive therapy to correct malformations in other organs.
(Chronic Non progressive Encephalopathy) • Brain injuries occur in the perinatal period and, less commonly, throughout infancy secondary to anoxia, hemorrhage, infection, and trauma. • The sudden onset of hypotonia in a previously well newborn or infant, with or without signs of encephalopathy, always suggests a cerebral cause. • Hypotonia is an early feature of meningitis in full-term and premature newborns.
Hypotonic cerebral palsy • Many hypotonic children due to causes in central nervous system are mentally retarded. • In atonic or hypotonic cerebral palsy, reflexes are brisk in spite of generalized flaccidity. • Floppy infant due to cerebral causes is associated with lethargy, poor feeding, and lack of alertness, poor Moro’s reflex, and seizures during the neonatal period.
Benign Congenital Hypotonia • The term benign congenital hypotonia is retrospective and refers to infants who are hypotonic at birth or shortly thereafter and later have normal tone. • It encompasses many different pathological processes that affect the brain, the motor unit, or both. • Most affected children have cerebral hypotonia. • An increased incidence of mental retardation, learning disabilities, and other sequalae of cerebral abnormality are evident later in life, despite the recovery of normal muscle tone.
Hypotonia in Children • SPINAL CORD • Spinal Cord Injury – Broken Neck • Spinal Muscular Atrophy • WERDNIG-HOFFMANN • INFECTIONS • Enterovirus - POLIO • Transverse Myelitis • MASS LESIONS
Spinal Cord Injury • Injuries in Breech Presentation • Injuries to the cervical spinal cord occur almost exclusively during vaginal delivery; • approximately 75% are associated with breech presentation and • 25% with cephalic presentation. • Because the injuries are always associated with a difficult and prolonged delivery, decreased consciousness is common, and hypotonia is falsely attributed to asphyxia or cerebral trauma. • Radiographs of the vertebrae show no abnormalities because bone displacement does not occur. MRI of the spine shows intraspinal edema and hemorrhage
Spinal Cord Injury • Injuries in Cephalic Presentation • Twisting of the neck during midforceps rotation causes high cervical cord injuries in cephalic presentation. • The trunk fails to rotate with the head. • The risk is greatest when amniotic fluid is absent because of delay from the time of membrane rupture to the application of forceps.
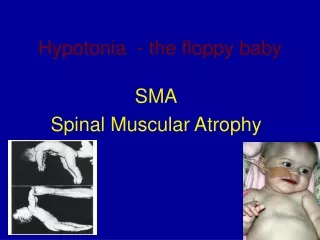
Werdning-Hoffman SyndromeSMA type 1 • Anterior Horn cell (neuronal) degeneration • Progressive Weakness: Proximal > Distal • Hypotonia • Areflexia • Atrophy / Fasciculations • Intact Brain Development
SMA • SMA is the second most common autosomal recessive diseasein the US after cystic fibrosis. • Incidence: • Type 1: 1 per 10,000 live births • Types II and III: 1 per 24,000 births • Worldwide 7.8-10 cases per 100,000 live births • ? M:F predominance or M>F • No ethnic predominance.
SMA • The genetic defects associated with SMA types I-III are localized on chromosome 5q11.2-13.3. • Mutations in the SMN gene result in a loss of function of the SMN protein. • Many classification systems based on inheritance, clinical, and genetic criteria.
SMA Type 1 • SMA type I, (Werdnig-Hoffmann acute infantile), occur birth – 6 months (95% by 3 months) • Severe, progressive muscle weakness and flaccid or reduced muscle tone (hypotonia). • Bulbar dysfunction includes poor suck ability, reduced swallowing, and respiratory failure. • Patients have no involvement of the extraocular muscles, and facial weakness is often minimal or absent. • They have no evidence of cerebral involvement, and infants appear alert.
SMA Type 1 • Impaired fetal movements are observed in 30% of cases • 60% of infants with SMA type I are floppy babies at birth. Prolonged cyanosis may be noted at delivery. • In some instances, the disease can cause fulminant weakness in the first few days of life. Such severe weakness and early bulbar dysfunction -> mean survival of 5.9 months. • Affected children never sit or stand. • In 95% of cases, infants die from complications of the disease by 18 months.
SMA Type 2 • SMA type II (chronic infantile, sitters) usually begin between 6 - 18 months. • Most common form of SMA • Most common manifestation is developmental motor delay. Infants with SMA type II often have difficulties with sitting independently or failure to stand by 1 year of age. • These children may learn to sit but will never be able to stand or walk.
SMA Type 2 • An unusual feature of the disease is a postural tremor affecting the fingers. This is thought to be related to fasciculations in the skeletal muscles • Pseudohypertrophy of the gastrocnemius muscle, musculoskeletal deformities, and respiratory failure can occur. • The lifespan of patients with SMA type II varies from 2 years to the third decade of life. Respiratory infections account for most deaths.
SMA Type 3 • SMA type III (Kugelberg-Welander, chronic juvenile, walkers) appear 18 months – adult. • Slowly progressive proximal weakness. Most can stand and walk but have trouble with motor skills, such as going up and down stairs. • Bulbar dysfunction occurs late in the disease. • Patients may show evidence of pseudohypertrophy. • The disease progresses slowly, and the overall course is mild. Many patients have normal life expectancies.
SMA • Congenital SMA with arthrogryposis (persistent contracture of joints with fixed abnormal posture of the limb) is a rare disorder. Manifestations include • severe contractures, • curvature of the spine, • chest deformity, • respiratory problems, • an unusually small jaw, and • drooping upper eyelids.
Poliovirus Infection • Small RNA virus : Neurotropic • Destroys neurons causing paralysis • Seasonal epidemics • Prodromal illness • Pain --> Asymmetric Paralysis • Rare but still occurs • vaccine related : 1 in 12 million • wild type due to groups refusing to vaccinate
MASS LESIONS OF SPINAL CORD • Rare • Intra-Abdominal Tumors • Neuroblastoma • Early in Infancy
PERIPHERAL NERVES • Polyneuropathy • Dysmylination • AUTOIMMUNE • CONGENITAL / GENETIC • Dysautonomia
MUSCLES CONGENITAL MYOPATHIES • DYSTROPHINOPATHIES • DUCHENNE’S • BECKER’S • CENTRAL CORE • MYOTUBULAR • NEMALINE ROD • MYOTONIC DYSTOPHY • Infantile Myositis
NEUROMUSCULAR JUNCTION • Toxins • Botulism • Myasthenia • Congenital • Neonatal transitory
INFANTILE BOTULISM • Infants usually 2 - 26 weeks old • Clostridium Botulinum --> Exotoxin • Prevents release of Acetylcholine • Cholinergic Blockade of skeletal muscle • Source of intestinal colonization usually unclear • Occurs mainly between March & October