Weakness and Hypotonia
760 likes | 1.11k Vues
Weakness and Hypotonia. Dr. William W. C. Young Pediatric Neurologist. Unending List of Causes of Weakness. Duchenne muscular dystrophy Becker’s muscular dystrophy Pompe’s disease McArdle’s disease Carnitine palmitoyl transferase deficiency Medium chain acyl-coA DHG def

Weakness and Hypotonia
E N D
Presentation Transcript
Weakness and Hypotonia Dr. William W. C. Young Pediatric Neurologist
Unending List of Causes of Weakness Duchenne muscular dystrophy Becker’s muscular dystrophy Pompe’s disease McArdle’s disease Carnitine palmitoyl transferase deficiency Medium chain acyl-coA DHG def Cushing’s disease Nemaline rod myopathy Dermato myositis Meningitis Hypoxic ischemic encephalopathy Cerebral palsy MELAS MERRF Adrenoleukodystrophy Gliomatosis cerebri Obstructive hydro cephalus Status epilepticus Substance abuse Uremia Liver failure Multiple sclerosis Hyothyroidism Tay Sach’s disease Botulism Myasthenia gravis Organophospha toxicity Magnesium toxicity Eaton Lambert syndrome Endplate AchR deficiency Endplate AchE deficiency Choline acetyl transferase deficiency Sea snake venom Gentamycin toxicity Viper venom Guillain Barre syndrome Diphtheria Vincristine neuropthy Diabetic neuropthy Polyarteritis nodosa Metachromatic leuko dystrophy Cockayne syndrome Charcot Marie Tooth disease Refsum’s disease Vitamin E deficiency Spinal muscular atrophy Poliomyelitis Werdnig Hoffman disease Kugelberg Welander disease Cold exposure Radiation sickness Fabry’s disease Herpes zoster Lyme disease Hepatitis B Porphyria Mechanical trauma Acromegaly Thallium toxicity Arsenic toxicity Syringomyelia Transverse myelitis C1-C2 sub luxation Spinal cord infarction Vertebral injury Spinal canal hematoma AV malform Tabes dorsalis Subacute combine degener Varicella myelopthy Syringobulbia Devic’s disease Acute Dissem EncephM
Systematic Neurologic Evaluation • Identify the problem accurately • Localize the lesion • Derive a differential diagnosis
e.g., Abnormal Movements • Identify the problem accurately • Seizures? • Dyskinesias? (tremors, tics, chorea) • Unsteadiness? • Stereotypic movements? • Localize the lesion • Derive a differential diagnosis
e.g., Abnormal Movements • Identify the problem accurately • Localize the lesion • Central or peripheral or spinal cord? • Nerve, neuromuscular junction, or muscle? • Derive a differential diagnosis
e.g., Abnormal Movements • Identify the problem accurately • Localize the lesion • Derive a differential diagnosis • Acute (infectious, traumatic, toxic-metabolic)
e.g., Abnormal Movements • Identify the problem accurately • Localize the lesion • Derive a differential diagnosis • Acute (epileptic, infectious, traumatic, toxic-metabolic, vascular-ischemic) • Chronic (endocrine, degenerative, neoplastic, chronic toxicity, nutritional, autoimmune, congenital, systemic)
Two Cases • Two year old female that is stumbling • 18 month old male that is not walking
Stumbling two year old female • Onset three days ago, unchanged • Recent respiratory infection 4 weeks ago • Prior history unremarkable • No toxic exposure, no recent travel, no adventure in the woods, no med use • No history of trauma • Normal developmental milestones
Stumbling two year old female • Speaking in short phrases • No dysmorphic features, normal head circ • Normal cranial nerves • No nystagmus, no unsteadiness • No abnormal movements • Normal reflexes • Decreased movements in left leg, pain in left calf with squeezing
Stumbling two year old female • Identify the problem accurately • Localize the lesion • Derive a differential diagnosis
Stumbling two year old female • Identify the problem accurately • Weakness
Stumbling two year old female • Identify the problem accurately • Weakness • Pain • Ataxia • Vertigo
Stumbling two year old female • Identify the problem accurately • Weakness in left leg • Pain in left calf • Ataxia • Vertigo
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Central • Spinal cord • Neuromuscular
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Central • Spinal cord • Neuromuscular (anterior horn cell, nerve, neuromuscular junction, muscle?)
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Central • Spinal cord • Neuromuscular (anterior horn cell, nerve, neuromuscular junction, muscle?)
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Neuromuscular (muscle—serum CK 2000) • Derive a differential diagnosis
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Neuromuscular (muscle—serum CK 2000) • Derive a differential diagnosis • Acute vs Chronic?
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Neuromuscular (muscle—serum CK 2000) • Derive a differential diagnosis • Acute (epileptic, infectious, traumatic, toxic-metabolic, vascular-ischemic)
Stumbling two year old female • Not Chronic • dystrophinopathy (Duchenne, Becker’s) • congenital myopathy (Nemaline rod, centronuclear) • inflammatory myopathy (dermatomyositis) • metabolic myopathy (MELAS, MERFF, MCAD def, CPT deficiency, Pompe’s, McArdle’s)
Stumbling two year old female • Differential diagnosis • anterior horn cell (poliomyelitis) • neuropathy (Guillain Barre syndrome) • neuromuscular junction (Myasthenic crisis, Botulism, organophosphate poisoning) • Muscle (trauma, inflammation, infection, ischemia)
Stumbling two year old female • Identify the problem accurately • Weakness and pain in left leg • Localize the lesion • Neuromuscular (muscle—serum CK 2000) • Derive a differential diagnosis • Acute (epileptic, infectious, traumatic, toxic-metabolic, vascular-ischemic) • POST INFECTIOUS MYOSITIS
Delayed walking 18 month male • No acute changes • Normal prenatal and birth history • No chronic medical problems, no meds • No hospitalizations, no surgeries • No toxic exposure, no recent travel, no adventure in the woods, no med use • No recent history of trauma or infection
Delayed walking 18 month male • Normal head size, no dysmorphic features, no neurocutaneous markers • Normal cranial nerves • Has 20 word vocabulary, understands verbal • No abnormal movements or postures • Cruising along furniture • Can appose thumbs to radii, can dorsiflex ankles, has vertical slip, some draping with horizont suspension • Normal reflexes, mild head lag
Delayed walking 18 month male • Identify the problem accurately • Localize the lesion • Determine the mechanism of action (to derive a reasonable differential diagnosis
Delayed walking 18 month male • Identify the problem accurately • Weakness • Pain • Ataxia • Vertigo
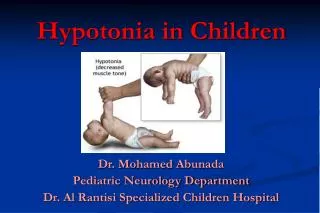
Delayed walking 18 month male • Identify the problem accurately • Not weak • Not pain • Not ataxic • No vertigo • Hypotonic
Delayed walking 18 month male • Identify the problem accurately • Weakness • Pain • Ataxia • Vertigo • Hypotonia? • Physiologic?
Delayed walking 18 month male • Identify the problem accurately • Hypotonia without weakness • Localize the lesion • Central • Spinal cord • Neuromuscular
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central (normal verbal and social development, normal head circ, no dysmorphic features, no neurocutaneous markers )
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central (normal verbal and social development, normal head circ, no dysmorphic features, no neurocutaneous markers ) • Not spinal cord (no paraplegia, no weakness)
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central (normal verbal and social development, normal head circ, no dysmorphic features, no neurocutaneous markers ) • Not spinal cord (no paraplegia, no weakness) • Neuromuscular? (no weakness, normal reflexes, normal muscle bulk)
Delayed walking 18 month male • Identify the problem accurately • Hypotonia without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Serum CK 40 normal • TSH normal • ESR 3 normal • Lactate 1.2 normal
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Derive a differential diagnosis • Acute vs chronic?
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Derive a differential diagnosis • Acute vschronic?
Delayed walking 18 month male • Differential diagnosis • Muscle (dystrophinopathy, congenital myopathy, inflammatory myopathy, metabolic myopathy) (Duchenne, Becker’s) • Neuromuscular junction (chronic Botulism, myasthenia, organophosphate poisoning) • Nerve (Guillain Barre syndrome, diphtheria, poliomyelitis, Charcot Marie Tooth) • Brain (genetic disorders, hypotonic cerebral palsy, microcephaly, macrocephaly, hypothyroidism)
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Derive a differential diagnosis • Acute vschronic?
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Derive a differential diagnosis • Acute vschronic? • Something distal to the muscle?
Delayed walking 18 month male • Identify the problem accurately • Hypotonic without weakness • Localize the lesion • Not central, not spinal cord, ?neuromuscular • Derive a differential diagnosis • Acute vschronic? • LIGAMENTOUS LAXITY • Physiologic • Ehlers Danlos syndrome, Cutis Laxa
Hypotonia (archaic terms) • Infantile progressive spinal muscular atrophy (Wernig 1891, Hoffman 1893) • Myotonia congenita (Oppenheim 1900) • Amyotonia congenita (Collier and Wilson 1908) • Benign congenital myopathy (Batten 1903, turner 1940) • Congenital universal muscular hypoplasia (Krabbe 1947) • Infantile muscular atrophy (Greenfield and Stern 1927) • Amyotonia congenita symptom complex (Brandt 1950) • Primary (essential) hypotonia (Sobel 1926) • Benign congenital hypotonia (Walton 1956)
Non-Neuromuscular Causes of Hypotonia • Disorders of the central nervous system • Connective tissue disorders • Genetic disorders • Metabolic; nutritional; endocrine
Non-Neuromuscular Causes of Hypotonia • Disorders of the central nervous system • Non-specific mental deficiency • Birth trauma, intracranial hemorrhage, neonatal hypoxic ischemic encephalopathy • Hypotonic cerebral palsy • Metabolic disorders; lipidoses; leukodystrophies, mucopolysaccharidoses, aminoacidurias, mitochondrial disorders
Non-Neuromuscular Causes of Hypotonia • Connective tissue disorders • Congenital laxity of ligaments • Ehlers-Danlos syndromes • Cutis laxa • Marfan syndrome • Osteogenesis imperfecta • Arachnodactyly • Loeys-Dietz syndrome • Camurati-Engelman syndrome
Ehlers Danlos syndromes • EDS I – severe • EDS II – mild • EDS III – hypermobile joints • EDS IV – vascular • EDS V – X linked type • EDS VI – ocular, scoliosis • EDS VII –arthrochalasis multiplex congenita • EDS VIII – periodontitis • EDS IX – copper transport disorder; X-linked cutis laxa • EDS X – fibronectin abnormality • EDS XI – familial hypermobility syndromes
Non-Neuromuscular Causes of Hypotonia • Genetic disorders • Down syndrome • Prader-Willi syndrome • Angelman syndrome • William syndrome • Miller-Dieker syndrome • Smith Lemli Opitz syndrome • Other structural chromosomal abnormalities