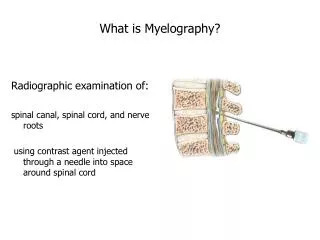
Myelography
Myelography. Dr Malith Kumarasinghe MBBS (Colombo). What is it?. Injection of intra-thecal contrast material to visualize disease or injury within the spinal column using CT and fluoroscopy Invasive test with associated risks

Myelography
E N D
Presentation Transcript
Myelography Dr Malith Kumarasinghe MBBS (Colombo)
What is it? • Injection of intra-thecal contrast material to visualize disease or injury within the spinal column using CT and fluoroscopy • Invasive test with associated risks • Has been largely replaced by MR, which is non-invasive and therefore safer
Why Is Myelography Still Used? • 10-20% of patients are unable to tolerated MR secondary to claustrophobia or the inability to remain still • Post-op metallic hardware (e.g. pedicle screws) and pacemakers cause distortion of MR images
Indications • Still considered the “gold standard” for degenerative disease • Confirmation of equivocal MR findings particularly in the cervical spine (such as small tumor nodules on nerve roots) • Used to visualize nerve roots in direct coronal plane to better assess degree of compression seen on MR • Often surgeons request myelography because they are more familiar with this technique
Indications (cont.) • Osteophytic disease is accurately identified owing to exquisite bone detail The left side of the spinal cord is compressed by an osteophyte
Indications (cont.) • Subarachnoid spread of tumor and small tumor implants on nerve roots • Arachnoiditis • Nerve root compression, extradural impressions, and disc protrusion • Visualization of dilated veins in patients with spinal A-V malformations Note: MR is the test of choice for visualizing the spinal cord and soft tissues if there is no contraindication
Contraindications • Patient with known severe hypersensitivity to contrast • Significant local or systemic infection where bacteremia is likely • Very recent prior myelogram (concern for contrast overdosage)
Pre-Procedure • Explain procedure to patient • Typically a lumbar approach is used to access the thecal sac since this is easier and has a lower complication rate • If patient has a complete block or lumbar access cannot be obtained it may be necessary to perform a cervical tap to analyze the cervical spine • Inform patient of risks (bleeding, HA, infection, pain, and seizure) and obtain consent • Stop all meds that lower seizure threshold (e.g. phenothiazines, antipschotics, tricyclic antidepressants, MAOIs, lithium, INH) 24 to 48 hrs prior to the procedure
Procedure • Follow lumbar puncture protocol (see appropriate section) • Once in the thecal sac CSF should be collected if it is needed for examination • Administer contrast (typically Omnipaque 300,240, 210, or 180) • Generally, 3.06g of iodinated contrast instilled intrathecally is the limit in adults (2.94g in children) • This corresponds to 10ml of contrast with a concentration of 300mg/ml or 12ml at 240mg/ml • Concentration in children should be less than 210mg/ml
Procedure – Lumbar myelogram • Contrast should be instilled with intermittent fluoroscopy to determine the correct amount to be administered (amount will vary depending on size of thecal sac) • AP, lateral and oblique films are obtained with patient in the prone position within 30 minutes after contrast injection (standing views may accentuate disk herniation) • Postmyelogram CT (several hours after administration of contrast) • Sections angled through the disks • Contiguous straight transaxial sections allow high-quality sagittal and coronal reconstruction
Lumbar Films(Lateral) Caudal termination of the subarachnoid space Spinous process of L3 L4 vertebral body Nerve roots of the cauda equina Sacral promontory
Lumbar Films(AP) Cauda Equina • sd L4 pedicle L4 spinal nerve Lateral extensions of subarachnoid space L5 spinal nerve S1 spinal nerve Caudal termination of subarachnoid space
Postmyelogram CT – Lumbar Sagittal reconstruction Axial
Procedure – Cervical Myelogram • Lumbar Approach • Easier, less patient anxiety, and lower complication rate when compared to cervical approach • Contrast is inserted as a bolus in the lumbar region of the spine and maintained as a bolus as the patient is tilted downward • Patient’s head is maintained in a hyperflexed fashion to prevent contrast from entering the intracranial sac • Once contrast is in the cervical region, the patient is flattened and the contrast pools in the natural lordosis of the cervical spine
Procedure – Cervical Myelogram • Cervical Approach • Reserved for patients with complete block or severe degenerative changes, scoliosis, or infection that prevent lumbar tap • Risk is increased (still low at .17 percent) owing to the presence of the spinal cord and vertebral arteries • Needle is inserted just anterior to the spinal lamina line at C1-C2 using cross-table lateral and AP fluoro • Needle is inched forward using lateral fluoro to ensure that the needle does not puncture the spinal cord • Permanent damage from puncturing the spinal cord is very rare unless contrast is injected into the cord itself. • Low dose contrast should be instilled into the thecal sac for cervical examination
Procedure – Cervical Myelogram • Obtain AP, lateral, and oblique films • Postmyelogram CT scans are obtained through suspicious levels seen on plain films • Sections angled through the disks • Contiguous straight transaxial sections allow high-quality sagittal and coronal reconstruction
Cervical Films Lateral AP
Postmyelogram CT – Cervical Axial section showing right-sided disk herniation Sagittal Reconstruction
Post-Procedure • Bed rest for 4 hrs • No heavy lifting or bending for 24 hrs • Keep head elevated to limit contrast flowing intracranially • Ibuprofen or Acetaminophen prn pain and HA • Resume restricted meds after 24 hrs