Download

1 / 15
150 likes | 255 Vues
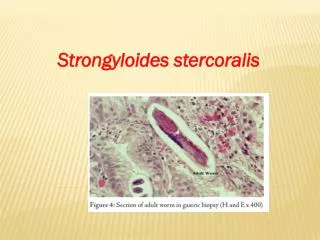
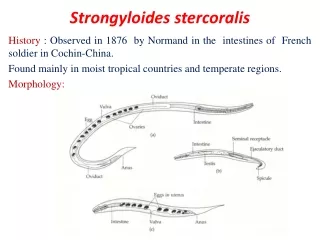
Strongyloides stercoralis in transplant patients. Alisa Alker. Life cycle. Geographic distribution. Over 50 million people are infected worldwide It endemic in Africa, parts of Asia, South America, Mexico, and the Southern US

E N D
Strongyloides stercoralis in transplant patients • Alisa Alker
Geographic distribution • Over 50 million people are infected worldwide • It endemic in Africa, parts of Asia, South America, Mexico, and the Southern US • National survey of 216,275 stool samples in 1987 found the prevalence of S. stercoralis to be 0.4% (CDC, 1991)
Clinical manifestations • diarrhea, abdominal pain, nausea, and vomiting • dry cough, dyspnea, transient pulmonary infiltrate, throat irritation, wheezing • Loffler syndrome (eosinophilic pneumonia) • fluctuating eosinophilia • rash (larva currens) • asymptomatic
Severe manifestations • Almost always found in immunocompromized hosts (associated with steroid use, HTLV, lymphoma, not HIV) • Hyperinfection and dissemination, leading to ileus, obstruction, GIB, pneumonitis, meningitis, peritonitis, UTI • the larvae bring with them bowel flora, leading to bacteremia, bacterial pneumonia, bacterial meningitis, etc • mortality is ~50% with treatment
Transplant patients • S. stercoralis has been reported in kidney (n=54), liver (n=3), lung (n=1), heart (n=3) and stem cell (n=7) transplant patients • More common for transplant patients to have hyperinfection, though more mild presentations have been reported • 0.7% of the renal transplant recipients between 1971-1984 at Vanderbilt had strongloidiasis (Morgan 1986)
Transplant patients • Strongloidiasis can be transmitted by solid organs and it has been documented in people who have not left the US • presentation more likely after transplantation or after treatment of acute rejection • associated with steroid use • cyclosporine may be protective • mortality rate in kidney transplant patients: 49% (Roxby 2009)
Diagnosis Roxby 2009
Treatment • ivermectin 200 ug/kg once daily for 2-3 days • thiabendazole 25 mg/kg twice daily for 3 days • more effective in killing the adult worms than the migrating larvae
Prevention • wearing shoes • improved sanitation • screening prior to transplantation?
References 1. Neva FA. Biology and immunology of human strongyloidiasis. J. Infect. Dis. 1986 Mar ;153(3):397-406. 2. Siddiqui AA, Berk SL. Diagnosis of Strongyloides stercoralis infection. Clin. Infect. Dis. 2001 Oct 1;33(7):1040-1047. 3. Segarra-Newnham M. Manifestations, diagnosis, and treatment of Strongyloides stercoralis infection. Ann Pharmacother. 2007 Dec ;41(12):1992-2001. 4. DeVault GA, King JW, Rohr MS, Landreneau MD, Brown ST, McDonald JC. Opportunistic infections with Strongyloides stercoralis in renal transplantation. Rev. Infect. Dis. 1990 Aug ;12(4):653-671. 5. Morgan JS, Schaffner W, Stone WJ. Opportunistic strongyloidiasis in renal transplant recipients. Transplantation. 1986 Nov ;42(5):518-524. 6. Marty FM. Strongyloides hyperinfection syndrome and transplantation: a preventable, frequently fatal infection. Transpl Infect Dis. 2009 Apr ;11(2):97-99. 7. Vilela EG, Clemente WT, Mira RRL, Torres HOG, Veloso LF, Fonseca LP, et al. Strongyloides stercoralis hyperinfection syndrome after liver transplantation: case report and literature review. Transpl Infect Dis. 2009 Apr ;11(2):132-136. 8. Roxby AC, Gottlieb GS, Limaye AP. Strongyloidiasis in transplant patients. Clin. Infect. Dis. 2009 Nov 1;49(9):1411-1423. 9. Mandell G, Bennett J, Dolin R. Principles and Practice of Infectious Diseases. 6th ed. Philadelphia, PA: Elsevier; 10. Center for Disease Control and Prevention. CDC surveillance summaries. MMWR. 1991 ;40(SS):