Oculocutaneous Albinism
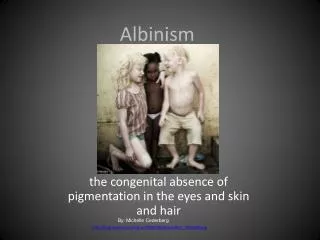
Oculocutaneous Albinism. Introduction. Albinism is a genetic disorder which is characterized by a defect in the gene that produces melanin . This results in a lack of pigmentation in the hair, skin and eyes (resulting in a white or pink color). types : OCA type 1.

Oculocutaneous Albinism
E N D
Presentation Transcript
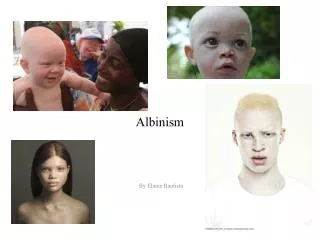
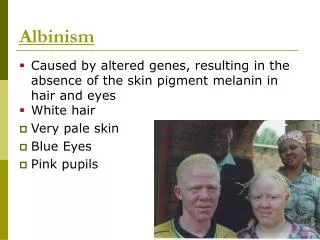
Introduction • Albinism is a genetic disorder which is characterized by a defect in the gene that producesmelanin. • This results in a lack of pigmentation in the hair, skin and eyes (resulting in a white or pink color).
types :OCA type 1 • OCA type 1A complete absence of pigment in the skin, the hair, and the eyes • (OCA type 1B)moderate pigmentation in these tissues • (OCA type 1TS), ie, temperature sensitive). pigment in hair follicles of the cooler areas of the body, such as the arms and the legs • Allforms of OCA type 1 also present with photophobia, moderate-to-severe reduced visual acuity, and nystagmus. The latter two ocular dysfunctions result from a misrouting of the optic fibers from the retina to the visual cortex
OCA type 2 • does not present with complete absence of pigment but rather manifests with a minimal-to-moderate amount of pigment remaining in the skin, the hair, and the eyes. • Many patients with OCA type 2 candeveloppigmented freckles, lentigines, and/or nevi with age. • The ocular presentations are similar to those in OCA type 1
OCA type 3 • manifests with minimal pigment reduction in the skin, the hair, and the eyes. This form of albinism was previously referred to as Rufous albinism and possibly Brown albinism. • The ocular presentations are similar to those in OCA type 1, but they are not as severe.
other • OCA type 4 manifests with a phenotype resembling OCA type 2 • OA manifests with ocular depigmentation and iris translucency. In addition, patients with OA present with congenital motor nystagmus that may be accompanied by reduced visual acuity, refractive errors, fundus hypopigmentation, lack of foveal reflex, and strabismus. Cutaneous depigmentation is not apparent
How is OCA type 1Inherited? • Albinism is an autosomal recessive trait. • An individual with albinism must inherit the albino gene from both of its parents. • This specific type is characterized by complete lack of tyrosinase activity because an inactive form of the enzyme is produced. • OCA1A is caused by mutations of the TYR gene that produce a inactive form of the tyrosinase enzyme.
The gene is located on chromosome 11 • The lack of this enzyme blocks the first step of the melanin biosynthetic pathway, and no melanin is formed in the appropriate melanocytes.
Others mutations • OCA type 2 results from mutation in the P gene • OCA type 3 results from mutation in the tyrosinase-related protein-1 (Tyrp1) gene, is inherited as an autosomal recessive trait. • OCA type 4 results from mutations in the membrane-associated transporter protein (MATP) • OA results from mutation in a gene on the X chromosome, is inherited as an X-linked recessive trait. The function of the OA gene product is unknown
Features/Symptoms • White or pink hair, skin, eyes • Eye problems: nystagmus (horizontal back and forth movement of eyes), strabismus (muscle imbalance, crossed eyes, lazy eye, protruding of eye), sensitivity to bright light and glare, far-sightedness, near-sightedness, astigmatism, fovealhypoplasia (retina does not develop normally prenatally or in infancy), nerve signals from retina to brain do not follow normal nerve routes, and iris cannot screen out light because of the lack of pigmentation. • Normal life span, same types of medical problems as non-albinos.
DX • The hair bulb tyrosinase assay has been used to differentiate between OCA type 1 and the other forms of albinism. scalp hair bulbs are gently plucked from the patient and placed in a 0.1% solution of (L-DOPA) for to 4 hours. If the sample is from a patient with OCA type 1, the hair bulbs remain white. In contrast, samples from all other forms of albinism turn dark during the period. • D/D: • Vitiligo • Piebaldism
RX • No treatment is available for hypopigmentation in the skin, the hair, or the eyes. • The use of broad-spectrum sunscreens and clothing is recommended to prevent ultraviolet-induced damage to the skin. • Visual impairment can be improved by using corrective lenses
Piebaldism • Autosomal dominant inheritence • Melanocytes are absent in affected area • Lesions present at birth • Depigmented macule present symmetrically with islands of normally pigmented or hyperpigmented macules withen the area of depigmented skin • Central parts of face, trunk and proximal parts of limbs are the common sites • RX:photoprotection,PUVA,Grafting
Hyperpigmentation Chloasma(melasma) • Etiology:hormonal factors, sunlight • Females >male • Age -30-50 • Brown macular pigmentation with well defined margins, it darkens with exposure to sun • Common sites:cheeks nose forehead and chin • RX: photoprotection, combination of topical hydroquinione,retinoic acid and topical corticosteroids ,chemical peeling with glycolic acid or trichloroacetic acid
Freckles • Autosomal dominant seen in fair individuals • Normal no. of melanocytes but hyperactive • Lesions are multiple brown macules which become darker on sun exposure • Individual macules may show variation in color • Face dorsolateral ,aspect of forearm and V of neck • RX: photoprotection,topicaldepigmenting agents like hydroquinone and azelaicacid, chemopeeling
Lentigines • Number of melanocytes are increased • May occur as a part of multisystem syndrome like PeutzJegher’s syndrome , etc or occur alone • Begins in childhood • Light brown to dark brown uniformly colored macules appearing at any part of the body including mucosa irrespective of photo exposure • RX : not required,facial lesions can be removed by excision or cryotherapy
Associations: PeutzJegher’ssyndrome:autosomal dominant • Scattered oral and acrallentigines • Small intestinal polyps and ovarian tumors Cronkhite-canada syndrome: • Multiple lentigines on dors of hands • Diffuse pigmentation of palms • Nail abnormalities • Alopecia • Intestinal polyposis