Understanding Malignant Melanoma: Risk Factors, Incidence, and Prevention Strategies
560 likes | 1.26k Vues
Malignant melanoma is a serious form of skin cancer originating from melanocytes, primarily affecting the skin but can also involve other tissues. It constitutes only 4% of skin cancer cases yet is responsible for the majority of skin cancer deaths globally. Early detection is crucial for improving survival rates, especially in high-risk populations. Factors such as fair complexion, sun exposure, and a history of moles significantly increase risk. Educational efforts in early detection can lead to better outcomes, especially in developed nations.

Understanding Malignant Melanoma: Risk Factors, Incidence, and Prevention Strategies
E N D
Presentation Transcript
MALIGNANT MELANOMA Özlem Akın, M.D. Yeditepe University Hospital Department of Dermatology
MALIGNANT MELANOMA • malignancy of pigment-producing cells (melanocytes) located predominantly in the skin, but also found in the eyes, ears, GI tract, leptomeninges, and oral and genital mucous membranes. • accounts for only 4% of all skin cancers; however, it causes the greatest number of skin cancer–related deaths worldwide. • early detection of thin cutaneous melanoma is the best means of reducing mortality.
MALIGNANT MELANOMA • Primary cutaneous melanoma may develop in precursor melanocytic nevi (ie, common, congenital, and atypical/dysplastic types), although more than 60% of cases are believed to arise de novo (ie, not from a preexisting pigmented lesion).
MALIGNANT MELANOMA • The development of melanoma is multifactorial and appears to be related to multiple risk factors, including • fair complexion • excessive childhood sun exposure and blistering childhood sunburns • an increased number of common and dysplastic moles • a family history of melanoma • the presence of a changing mole or evolving lesion on the skin • older age
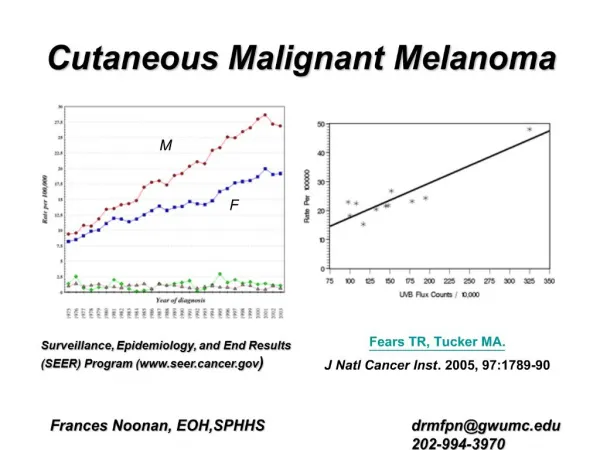
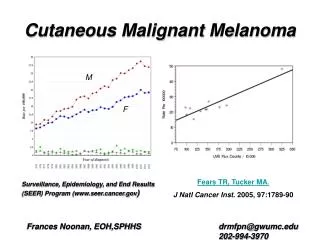
MALIGNANT MELANOMA • incidence has more than tripled in the white population during the last 20 years • currently is the sixth most common cancer in the United States • current lifetime risk for developing invasive melanoma is 1 case per 60 Americans, a 2000% increase since 1930. • this risk rises to 1 case per 32 Americans if noninvasive melanoma in situ is included.
MALIGNANT MELANOMA • incidence has continued to increase worldwide, with the highest incidence in Australia and New Zealand • the most recent analysis of global cancer statistics, from 2002, demonstrated a prevalence of 37.7 cases per 100,000 men and 29.4 cases per 100,000 women in Australia and New Zealand, compared with 6.4 cases per 100,000 men and 11.7 cases per 100,000 women in North America
MALIGNANT MELANOMA • Individuals with cutaneous melanoma have higher survival rates in developed countries (91% in US SEER registries and 81% in Europe) than in developing countries (approximately 40%). • Increased educational efforts in developed areas result in earlier diagnosis, treatment, and potential cure of thinner lesions.
MALIGNANT MELANOMA • primarily a malignancy of white individuals. • African American persons develop melanoma approximately one twentieth as frequently as white persons, and the prevalence in Hispanic persons is approximately one sixth of that in white persons. • However, mortality rates are higher in African Americans and Hispanics, who are more likely to have acral melanoma and advanced disease at presentation.
MALIGNANT MELANOMA • In the United States, invasive melanoma has a higher female predilection from birth to age 39 years (1 in 389 women compared with 1 in 656 men). • However, from age 40 years and older, melanoma in men predominates, occurring in 1 in 41 men compared with 1 in 61 women over a lifetime. • Worldwide, of the 160,000 new cases estimated to have occurred in 2002, women were affected slightly more than men (male-to-female ratio, 0.97:1). • Conversely, of the estimated 41,000 worldwide deaths in 2002, more occurred in men than in women (male-to-female ratio 1.2:1).
MALIGNANT MELANOMA • The median age at melanoma diagnosis is 53 years; • however, it is the most common cancer in women aged 25-29 years and is second only to breast cancer in women aged 30-34 years. • The most striking differences in melanoma incidence and mortality occur in individuals older than 65 years, although modest differences in age-specific incidence and mortality are notable in persons older than 50 years.
MALIGNANT MELANOMA • Older individuals are both more likely to acquire and to die from melanoma; • thus, elderly persons should be a primary target for secondary melanoma prevention, including early detection and screening. • Treatment options in elderly persons may also be limited because of comorbid medical conditions, an inability to tolerate adverse medication effects or toxicity, the increased likelihood of drug interactions, and potential exclusion from clinical trials based on age criteria.
MALIGNANT MELANOMA • A new or changing mole or blemish is the most common warning sign for melanoma. • Variation in color and/or an increase in diameter, height, or asymmetry of borders of a pigmented lesion are noted by more than 80% of patients with melanoma at the time of diagnosis. • Symptoms such as bleeding, itching, ulceration, and pain in a pigmented lesion are less common but warrant an evaluation. • because the majority of cutaneous melanoma arises de novo (ie, not in association with a precursor nevus), the wholesale removal of melanocytic nevi is not warranted for melanoma prevention. • However, individuals with numerous moles (common or dysplastic) or a family history of melanoma should be educated regarding the importance of skin self-examination for early detection of skin cancer.
MALIGNANT MELANOMA • The ABCDE criteria : • Asymmetry: Half the lesion does not match the other half. • Border irregularity: The edges are ragged, notched, or blurred. • Color variegation: Pigmentation is not uniform and may display shades of tan, brown, or black; white, reddish, or blue discoloration is of particular concern. • Diameter: A diameter greater than 6 mm is characteristic, although some melanomas may have smaller diameters; any growth in a nevus warrants an evaluation. • Evolving: Changes in the lesion over time are characteristic; this factor is critical for nodular or amelanotic (nonpigmented) melanoma, which may not exhibit the classic criteria above.
MALIGNANT MELANOMA • Four major clinicopathologic (or histogenetic) subtypes of primary cutaneous melanoma have been identified: • superficial spreading melanoma • nodular melanoma • lentigo maligna melanoma • acral lentiginous melanoma. • Distinction among the subtypes is based on histologic growth pattern, anatomic site, and degree of sun damage. • The pattern of sun exposure varies between the types (sustained in lentigo maligna vs intermittent in superficial spreading). • Whether the melanoma subtype affects the overall prognosis remains controversial.
MALIGNANT MELANOMA • With the exception of nodular melanoma, the growth patterns of the other subtypes are characterized by a preceding in situ (radial growth) phase that lacks the biologic potential to metastasize and may last from months to years before dermal invasion occurs. • While all in situ melanoma may not necessarily progress to invasive melanoma, complete excision is recommended to prevent invasion and effect cure.
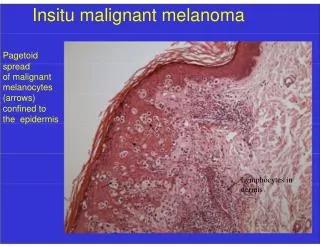
Superficial spreading melanoma • most common on the trunk in men and on the legs in women • most commonly seen in individuals aged 30-50 years • manifests as a flat or slightly elevated brown lesion with variegate pigmentation (ie, black, blue, pink, or white discoloration) • generally greater than 6 mm in diameter. • Irregular asymmetric borders are characteristic • Histologically, it is characterized by buckshot (pagetoid) scatter of atypical melanocytes within the epidermis
Superficial spreading melanoma, left breast, 1.3-mm Breslow depth.
Nodular melanoma • occurs in 15-30% of patients • seen most commonly on the legs and trunk • Rapid growth occurs over weeks to months; this subtype is responsible for most thick melanomas • manifests as a dark brown-to-black papule or dome-shaped nodule, which may ulcerate and bleed with minor trauma; it may be clinically amelanotic (ie, not pigmented). • tends to lack the typical ABCDE melanoma warning signs and, thus, may elude early detection. • More commonly, it exhibits elevation, ulceration with bleeding, or both at presentation. • Histologically, it lacks a radial growth phase.
Lentigo maligna melanoma • The incidence of lentigo maligna subtypes (in situ and invasive) appears to be rising in the United States. • typically located on the head, neck, and arms (chronically sun-damaged skin) of fair-skinned older individuals (average age 65 y). • It grows slowly over 5-20 years. • The in situ precursor lesion is usually large (>1-3 cm in diameter), present for a minimum of 10-15 years, and demonstrates macular pigmentation ranging from dark brown to black, although hypopigmented (white) areas are common within lentigo maligna. • Dermal invasion (progression to lentigo maligna melanoma) is characterized by the development of raised blue-black nodules within the in situ lesion. • Histologically, it is characterized by a predominantly junctional confluent proliferation of melanocytes and extension along adnexal structures. • Solar elastosis is typically prominent.
Lentigo maligna melanoma, right lower cheek. Centrally located erythematous papule represents invasive melanoma with surrounding macular lentigo maligna (melanoma in situ)
Acral lentiginous melanoma • least common subtype (2-8% of cases in white persons). • accounts for 29-72% of melanoma cases in dark-skinned individuals (ie, African American, Asian, and Hispanic persons) and, because of delays in diagnosis, may be associated with a worse prognosis. • occurs on the palms, on the soles, or beneath the nail plate (subungual variant) • Subungual melanoma may manifest as diffuse nail discoloration or a longitudinal pigmented band within the nail plate. • must be differentiated from a benign junctional melanocytic nevus of the nail bed, which has a similar appearance. • Pigment spread to the proximal or lateral nail folds is termed the Hutchinson sign, which is a hallmark for acral lentiginous melanoma.
Acral lentiginous melanoma (1-mm Breslow depth), left sole. Diagnostic punch biopsy site is located superiorly
Cutaneous melanoma with characteristic asymmetry, irregular borders, and color variation
MALIGNANT MELANOMA • Rare melanoma variants (<5% of melanomas) • (1) desmoplastic/neurotropic melanoma • (2) mucosal (lentiginous) melanoma • (3) malignant blue nevus • (4) melanoma arising in a giant congenital nevus • (5) melanoma of soft parts (clear cell sarcoma)
Amelanotic melanoma • <5% of melanomas • nonpigmented and, clinically, appears pink or flesh-colored, often mimicking basal cell or squamous cell carcinoma or a ruptured hair follicle. • occurs most commonly in the setting of the nodular melanoma subtype or melanoma metastasis to the skin, presumably because of the inability of these poorly differentiated cancer cells to synthesize melanin pigment.
MALIGNANT MELANOMA • Primary risk factors for or clinical warning signs of melanoma: • Changing mole (most important clinical warning sign) • Clinical atypical/dysplastic nevi (particularly >5-10) • Large numbers of common nevi (>100) • Large (giant) congenital nevi (>20 cm diameter in an adult) • Previous melanoma • Sun sensitivity/history of excessive sun exposure • Melanoma in first-degree relative(s) • Prior nonmelanoma skin cancer (basal cell and squamous cell carcinoma) • Male sex • Age older than 50 years • Presence of xeroderma pigmentosum or familial atypical mole melanoma syndrome: These 2 genodermatoses confer a 500- to 1000-fold greater relative risk of developing melanoma.
MALIGNANT MELANOMA • Superficial spreading melanoma tends to occur at sites of intermittent, intense sun exposure (ie, on trunk in males and legs and back in females) • Lentigo maligna melanoma is more prevalent on the chronically sun-damaged skin of the head, neck, and arms • The disease shows an increased worldwide incidence in fair-complexioned individuals living in sunny climates and nearer the equator, suggesting a causative role for ultraviolet radiation.
MALIGNANT MELANOMA • A fair-skin phenotype (blue/green eyes, blond or red hair, light complexion, sun sensitivity) • occurrence of blistering sunburn(s) in childhood and adolescence are universal risk factors • Individuals with these traits have been the focus of preventive efforts worldwide. • Pregnancy or hormonal therapy with oral contraceptives or hormone replacement does not appear to be a risk factor
Differential Diagnoses • Atypical Mole (Dysplastic Nevus) • Lentigo • Basal Cell Carcinoma • Metastatic Carcinoma of the Skin • Blue Nevi • Nevi of Ota and Ito • Cherry Hemangioma • Melanocytic Nevi • Dermatofibroma • Seborrheic Keratosis • Halo Nevus • Spitz Nevus • Keloid and Hypertrophic Scar • Squamous Cell Carcinoma • Keratoacanthoma • Vitiligo • Chronic paronychia (for subungual melanoma) • Subungual hematoma (for subungual melanoma) • Melanonychia striata (for subungual melanoma) • Traumatized nevus (for superficial spreading or nodular subtypes)
Laboratory Studies • The most important aspects of the initial workup are a careful history, review of systems, and physical examination. • Sentinel lymph node biopsy (SLNB) is generally indicated for pathologic staging of the regional nodal basin(s) for primary tumors greater than or equal to 1 mm depth and when certain high-risk histologic features (eg, ulceration, extensive regression, high mitotic rate, angiolymphatic invasion) are present in thinner melanomas. • Published data have shown that baseline and surveillance laboratory studies (eg, lactate dehydrogenase [LDH] level, liver function tests), chest radiography (CXR), and other imaging studies (eg, CT scanning, positron emission tomography [PET] scanning, bone scanning, MRI) are not typically beneficial for stage I/II (cutaneous) melanoma patients without signs or symptoms of metastasis. • A metastatic workup should be initiated if physical findings or symptoms suggest disease recurrence or if the patient has documented nodal metastasis based on results from the SLNB.
Laboratory Studies • Serum LDH levels have been incorporated into the American Joint Committee on Cancer (AJCC) 2002 melanoma staging guidelines for the classification of stage IV (distant) disease • Elevated LDH levels are associated with worse survival in this subgroup • Serum S-100 protein levels may also be useful as a tumor marker in patients with metastatic disease • Baseline metastatic staging for melanoma patients with primary tumors greater than 1 mm in depth may include CXR, which typically is repeated every 6-12 months for routine surveillance (optional in the absence of signs or symptoms of metastatic disease)
Procedures • The criterion standard for melanoma diagnosis is histopathologic examination of clinically suggestive skin or mucosal lesions. • An excisional biopsy with narrow margins is preferred when possible. • In the case of lentigo maligna, a broad, paper-thin shave biopsy or multiple smaller biopsies may be the best techniques. • The biopsy report should generally include the following: • Tumor thickness (Breslow depth) • Presence of ulceration • Anatomic level of invasion (Clark level) • Presence of mitoses • Presence of regression (associated with lower rates of sentinel node positivity and improved disease-free survival) • Lymphatic/vessel (lymphovascular) invasion or vascular involvement • Host response (tumor-infiltrating lymphocytes)
Procedures • Immunohistochemical staining for lineage (S-100, homatropine methylbromide 45 [HMB-45], melan-A/Mart-1) or proliferation markers (proliferating cell nuclear antigen, Ki67) may be helpful in some cases for histologic differentiation from melanoma simulators • evidence of lack of maturation with HMB-45 staining and patchy, rather than diffuse, staining with S-100 may be helpful for distinguishing spitzoid melanoma from Spitz nevus.
Procedures • when an excisional biopsy is performed, 1-3 mm of normal skin surrounding the pigmented lesion should be removed to provide accurate diagnosis and histologic microstaging. • Wider margins (>1 cm) could theoretically disrupt afferent cutaneous lymphatic flow and affect the ability to identify the sentinel node(s) accurately in patients eligible for this staging procedure. • Some data, however, suggest that accurate mapping is possible after wider excision. • Superficial shave biopsies of suggestive pigmented lesions are discouraged because partial removal of the primary melanoma may not provide an accurate measurement of tumor thickness, which is the most important histologic prognostic factor for cutaneous melanoma.
Treatment • Surgery is the primary mode of therapy for localized cutaneous melanoma. • Numerous adjuvant therapies have been investigated for the treatment of localized cutaneous melanoma following complete surgical removal. • No survival benefit has been demonstrated for adjuvant chemotherapy, nonspecific (passive) immunotherapy, radiation therapy, retinoid therapy, vitamin therapy, or biologic therapy. • Adjuvant interferon (IFN) alfa-2b is the only adjuvant therapy approved by the US Food and Drug Administration for high-risk melanoma (currently defined as stages IIB, IIC, and III), which is associated with a 40-80% chance of relapse and death. • Various experimental melanoma vaccines also show promise in the adjuvant setting.
Treatment • Surgical margins for primary melanoma • The narrowest efficacious margins for cutaneous melanoma have yet to be determined. • melanoma in situ → 5 mm, • melanomas up to 1 mm in depth→ 1 cm • intermediate thickness (1-4 mm Breslow depth)→ 2 cm • melanomas greater than 4 mm in thickness (high-risk primaries) → 2 cm
Treatment • Mohs surgery may have certain "niche" indications, including melanomas located the head, neck, hands, or feet. • Mohs surgery may prove useful in completely removing subclinical tumor extension in certain subtypes of melanoma in situ, such as lentigo maligna and acral lentiginous melanoma in situ. • prospective randomized clinical trials have shown no survival benefit for elective lymphadenectomy for melanomas of varying thicknesses on the extremities and marginal, if any, benefit for nonextremity melanomas
Treatment • Lymphatic mapping and sentinel node biopsy have effectively solved the dilemma of whether to perform regional lymphadenectomy (in the absence of clinically palpable nodes) in patients with thicker melanomas (≥1 mm in depth) and in those of less than 1 mm depth with adverse features (eg, ulceration, lymphovascular invasion, mitotic rate ≥ 1 mm2).
Treatment • Preoperative radiographic mapping (lymphoscintigraphy) and vital blue dye injection around the primary melanoma or biopsy scar (at the time of wide local excision/reexcision) is performed to identify and remove the initial draining regional node(s). • The sentinel node is examined for the presence of micrometastasis using both routine histology and immunohistochemistry; if present, a therapeutic or completion lymph node dissection (CLND) is performed. • A negative sentinel node biopsy result prevents the morbidity associated with an unnecessary lymphadenectomy. • Sentinel node status (positive or negative) is the most important prognostic factor for recurrence and is the most powerful predictor of survival in melanoma patients.