Download
1 / 1
10 likes | 12 Vues
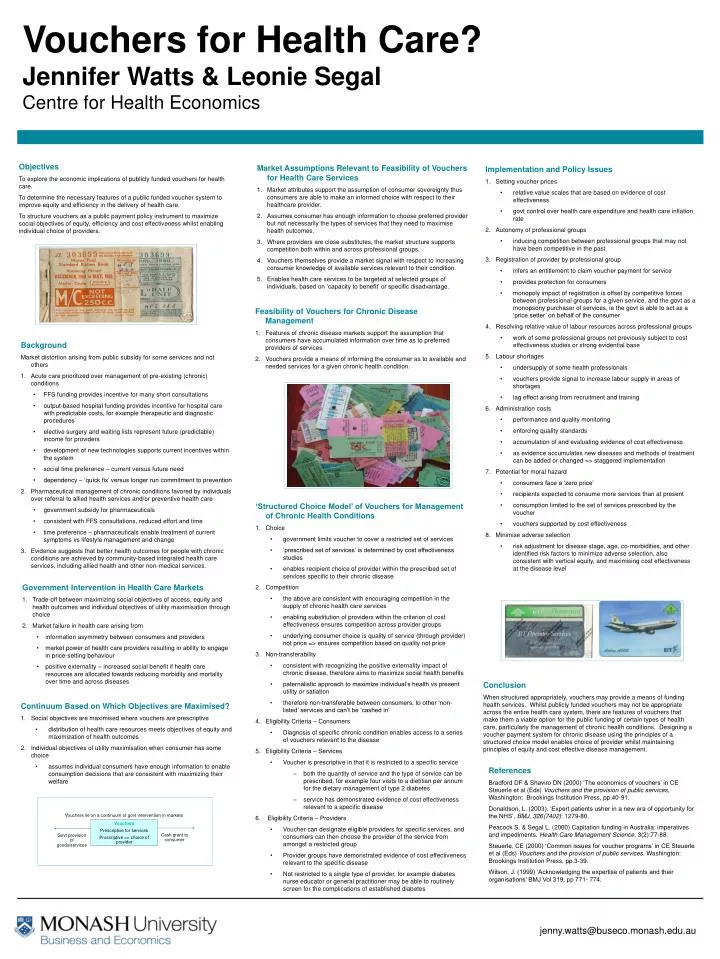
This study explores the economic implications of publicly funded vouchers for health care and aims to improve equity and efficiency in the delivery of health care services. It examines the necessary features of a public funded voucher system and its potential impact on social objectives of equity, efficiency, and cost effectiveness, while enabling individual choice of providers.

E N D
Vouchers lie on a continuum of govt intervention in markets Vouchers Prescriptive for services Proscriptive => choice of provider Cash grant to consumer Govt provision of goods/services Vouchers for Health Care?Jennifer Watts & Leonie SegalCentre for Health Economics Objectives To explore the economic implications of publicly funded vouchers for health care. To determine the necessary features of a public funded voucher system to improve equity and efficiency in the delivery of health care. To structure vouchers as a public payment policy instrument to maximize social objectives of equity, efficiency and cost effectiveness whilst enabling individual choice of providers. • Market Assumptions Relevant to Feasibility of Vouchers for Health Care Services • Market attributes support the assumption of consumer sovereignty thus consumers are able to make an informed choice with respect to their healthcare provider. • Assumes consumer has enough information to choose preferred provider but not necessarily the types of services that they need to maximise health outcomes. • Where providers are close substitutes, the market structure supports competition both within and across professional groups. • Vouchers themselves provide a market signal with respect to increasing consumer knowledge of available services relevant to their condition. • Enables health care services to be targeted at selected groups of individuals, based on ‘capacity to benefit’ or specific disadvantage. • Implementation and Policy Issues • Setting voucher prices • relative value scales that are based on evidence of cost effectiveness • govt control over health care expenditure and health care inflation rate • Autonomy of professional groups • inducing competition between professional groups that may not have been competitive in the past • Registration of provider by professional group • infers an entitlement to claim voucher payment for service • provides protection for consumers • monopoly impact of registration is offset by competitive forces between professional groups for a given service, and the govt as a monopsony purchaser of services, ie the govt is able to act as a ‘price setter’ on behalf of the consumer • Resolving relative value of labour resources across professional groups • work of some professional groups not previously subject to cost effectiveness studies or strong evidential base • Labour shortages • undersupply of some health professionals • vouchers provide signal to increase labour supply in areas of shortages • lag effect arising from recruitment and training • Administration costs • performance and qualitymonitoring • enforcing quality standards • accumulation of and evaluating evidence of cost effectiveness • as evidence accumulates new diseases and methods of treatment can be added or changed => staggered implementation • Potential for moral hazard • consumers face a ‘zero price’ • recipients expected to consume more services than at present • consumption limited to the set of services prescribed by the voucher • vouchers supported by cost effectiveness • Minimise adverse selection • risk adjustment for disease stage, age, co-morbidities, and other identified risk factors to minimize adverse selection, also consistent with vertical equity, and maximising cost effectiveness at the disease level • Feasibility of Vouchers for Chronic Disease Management • Features of chronic disease markets support the assumption that consumers have accumulated information over time as to preferred providers of services. • Vouchers provide a means of informing the consumer as to available and needed services for a given chronic health condition. • Background • Market distortion arising from public subsidy for some services and not others • Acute care prioritized over management of pre-existing (chronic) conditions • FFS funding provides incentive for many short consultations • output-based hospital funding provides incentive for hospital care with predictable costs, for example therapeutic and diagnostic procedures • elective surgery and waiting lists represent future (predictable) income for providers • development of new technologies supports current incentives within the system • social time preference – current versus future need • dependency – ‘quick fix’ versus longer run commitment to prevention • Pharmaceutical management of chronic conditions favored by individuals over referral to allied health services and/or preventive health care • government subsidy for pharmaceuticals • consistent with FFS consultations, reduced effort and time • time preference – pharmaceuticals enable treatment of current symptoms vs lifestyle management and change • Evidence suggests that better health outcomes for people with chronic conditions are achieved by community-based integrated health care services, including allied health and other non-medical services. • ‘Structured Choice Model’ of Vouchers for Management of Chronic Health Conditions • Choice • government limits voucher to cover a restricted set of services • ‘prescribed set of services’ is determined by cost effectiveness studies • enables recipient choice of provider within the prescribed set of services specific to their chronic disease • Competition • the above are consistent with encouraging competition in the supply of chronic health care services • enabling substitution of providers within the criterion of cost effectiveness ensures competition across provider groups • underlying consumer choice is quality of service (through provider) not price => ensures competition based on quality not price • Non-transferability • consistent with recognizing the positive externality impact of chronic disease, therefore aims to maximize social health benefits • paternalistic approach to maximize individual’s health vs present utility or satiation • therefore non-transferable between consumers, to other ‘non-listed’ services and can’t be ‘cashed in’ • Eligibility Criteria – Consumers • Diagnosis of specific chronic condition enables access to a series of vouchers relevant to the disease • Eligibility Criteria – Services • Voucher is prescriptive in that it is restricted to a specific service • both the quantity of service and the type of service can be prescribed, for example four visits to a dietitian per annum for the dietary management of type 2 diabetes • service has demonstrated evidence of cost effectiveness relevant to a specific disease • Eligibility Criteria – Providers • Voucher can designate eligible providers for specific services, and consumers can then choose the provider of the service from amongst a restricted group • Provider groups have demonstrated evidence of cost effectiveness relevant to the specific disease • Not restricted to a single type of provider, for example diabetes nurse educator or general practitioner may be able to routinely screen for the complications of established diabetes • Government Intervention in Health Care Markets • Trade-off between maximizing social objectives of access, equity and health outcomes and individual objectives of utility maximisation through choice • Market failure in health care arising from • information asymmetry between consumers and providers • market power of health care providers resulting in ability to engage in price-setting behaviour • positive externality – increased social benefit if health care resources are allocated towards reducing morbidity and mortality over time and across diseases Conclusion When structured appropriately, vouchers may provide a means of funding health services. Whilst publicly funded vouchers may not be appropriate across the entire health care system, there are features of vouchers that make them a viable option for the public funding of certain types of health care, particularly the management of chronic health conditions. Designing a voucher payment system for chronic disease using the principles of a structured choice model enables choice of provider whilst maintaining principles of equity and cost effective disease management. • Continuum Based on Which Objectives are Maximised? • Social objectives are maximised where vouchers are prescriptive • distribution of health care resources meets objectives of equity and maximization of health outcomes • Individual objectives of utility maximisation when consumer has some choice • assumes individual consumers have enough information to enable consumption decisions that are consistent with maximizing their welfare References Bradford DF & Shaviro DN (2000) ‘The economics of vouchers’ in CE Steuerle et al (Eds) Vouchers and the provision of public services, Washington: Brookings Institution Press, pp.40-91. Donaldson, L. (2003). ‘Expert patients usher in a new era of opportunity for the NHS’, BMJ, 326(7402): 1279-80. Peacock S. & Segal L. (2000) Capitation funding in Australia: imperatives and impediments. Health Care Management Science. 3(2):77-88. Steuerle, CE (2000) ‘Common issues for voucher programs’ in CE Steuerle et al (Eds) Vouchers and the provision of public services, Washington: Brookings Institution Press, pp.3-39. Wilson, J. (1999) ‘Acknowledging the expertise of patients and their organisations’ BMJ Vol 319, pp 771- 774. jenny.watts@buseco.monash.edu.au