Download
1 / 55
550 likes | 630 Vues
#1008 New Strategies in Treatment of Lung Cancer. November 9 to 12 Patrick Ross, Jr. MD, PhD Assistant Professor of Surgery Division of Surgical Thoracic Oncology The Ohio State University Medical Center & The James Cancer Hospital and Solove Research Institute Gregory A. Otterson, MD

E N D
#1008New Strategies in Treatment of Lung Cancer November 9 to 12 Patrick Ross, Jr. MD, PhD Assistant Professor of Surgery Division of Surgical Thoracic Oncology The Ohio State University Medical Center & The James Cancer Hospital and Solove Research Institute Gregory A. Otterson, MD Associate Professor of Internal Medicine Division of Hematology and Oncology The Ohio State University Medical Center & The James Cancer Hospital and Solove Research Institute
Gregory A. Otterson, MDAssociate Professor of Internal MedicineDivision of Hematology and OncologyThe Ohio State University Medical Center &The James Cancer Hospital and Solove Research Institute 1
Profile Mr. Perkins • 55 year old male • Smoker • Hemoptosis • Photodynamic therapy • 2 cycles of chemotherapy Diagnosis: Large T3 N2 tumor 2
New Treatment Strategies InThe Treatment Of Lung Cancer • Multimodality treatment for locally advanced NSCLC - Surgery - Radiation - Chemotherapy • Novel agents - SCLC - antisense bcl2 - NSCLC - farnesyltransferase inhibitors 4
Lung Cancer Statistics,1999 • Greatest cause of cancer death worldwide - 921,000 deaths worldwide - 158,900 US deaths (90,900 men, 68,000 women) • 28% of US cancer deaths (14% cancer cases) 5
Lung Cancer Treatment -Stage And Type Specific • Non-small cell lung cancer (NSCLC) - ~80% of lung cancer - Principally surgically treated - Chemotherapy and radiation therapy added in specific circumstances • Small cell lung cancer (SCLC) - ~20% of lung cancer - Principally chemotherapy +/- radiation therapy 6
Locally Advanced NSCLC • Stage IIIB - Generally unresectable - Either bulky primary tumor involving critical mediastinal structures, pleural effusion or contralateral mediastinal lymph node involvement • Chemotherapy added to radiation therapy improves control and survival - Concurrent vs. sequential? 7
Locally Advanced NSCLC • Stage IIIA - Theoretically resectable - Ipsilateral mediastinal lymph nodes involved • Surgery is principal modality in most centers - Post-operative radiation improves local controls - Post-operative chemotherapy has not been dramatically successful 8
Stage IIIA NSCLC • Questions asked in clinical trials - ? Pre-op chemotherapy - ? Pre-op radiation therapy - ? Pre-op chemo-radiotherapy - ? Role of surgery • These questions remain open 9
Stage IIIA NSCLC • Balance risks with benefits of aggressive treatment - Improved local / systemic control - Increased treatment related morbidity and mortality with combined treatment • Prognostic / treatment factors - Weight loss (5-10%), performance status, age, comorbid conditions 10
OSU Trial For ResectableStage IIIA NSCLC • Pre-operative chemotherapy for three cycles (paclitaxel and carboplatin) • Pre-operative radiation (to 4500 cGy) with a novel (Gadolinium-Texaphyrin) radiation sensitizer • Curative resection planned after completion of radiation • If incomplete resection, post-op radiation 11
Novel Drug Strategies • Apoptosis - many chemotherapeutic drugs induce cell death by initiating a cellular suicide pathway in cancer cells (called apoptosis) • Some cancers (including most SCLC) overexpress an oncogene (bcl2) that protects cells from apoptosis 12
Bcl2 Family Of Proteins • Family of proteins that are involved in apoptotic pathways (some pro-, others anti-apoptotic) • Bcl2 family members can homo- and hetero-dimerize with each other • Susceptibility to programmed cell death (apoptosis) depends on relative ratio of homo- and hetero-dimers 13
Bcl2 Antisense Therapy • Chemotherapy induces cell death through apoptosis • Bcl2 protects cells from apoptotic death • In theory, chemotherapy should be more effective if bcl2 is inhibited • Therefore, use bcl2 antisense (synthetic oligonucleotide directed against the bcl2 messenger RNA molecule) 15
Bcl2 Antisense In SCLC • Patient population: resistant SCLS (Either progressive disease on treatment or relapse within 3 months) • G3139 (bcl2 antisense) via continuous IV infusion X 7 days • Paclitaxel 175 mg / m2 over 3 hours, day 6 q 3 weeks 17
Novel Drug Strategies • Ras is an oncogene that is mutated in many different cancers (~90% of pancreatic ca, ~50% of colon ca and ~30% of NSCLC) • Ras (normal and mutant) requires association with the cell membrane via a cholesterol precurser for activity 18
Inhibit Ras Activity ThroughIts Membrane Association • HMG-CoA reductase inhibitors were attempted without remarkable success • Inhibition of the farnesyl-transferase enzyme has been pursued with better pre-clinical ad early clinical activity • Single agent and combination trials are now underway(including one at OSU) 20
Improvement InLung Cancer Survival? • Better local control - Improved surgical technique - Improved preparation / selection of surgical patients - Improved radiotherapy technique and radiation sensitizers 21
Improvement InLung Cancer Survival? • Better control of systemic disease - Application of current chemotherapeutic agents in combination with surgery and / or radiation therapy - Novel chemotherapeutic agents, designed to attack specific genetic defects in tumor cells (for example, bcl2 antisense and farnesyltransferase inhibitors) 22
Summary Mr. Perkins Diagnosis: IIIA non-small lung cancer Treatment: - Photodynamic therapy - Chemotherapy - Right pneumonectomy Follow-up: - Operation went smoothly - Further radiation and chemotherapy Prognosis: Good 24
Patrick Ross, Jr. MD, PhD Assistant Professor of Surgery Division of Surgical Thoracic Oncology The Ohio State University Medical Center & The James Cancer Hospital and Solove Research Institute 25
Profile Joseph Tigerina • 61 year old male • Former smoker • Newly identified left upper lobe mass • Presented to family physician with left shoulder and back pain 26
Profile Joseph Tigerina Symptoms - No cough or hemoptsis - Some fatigue - No weight loss Evaluation - CT scan and CT needle guided biopsy - MRI - PET scan Diagnosis: Non small cell carcinoma 26-A
Non Small CellLung Cancer • Can the tumor be resected? • Can the patient undergo resection? • What can be done to improve the outcome? 28
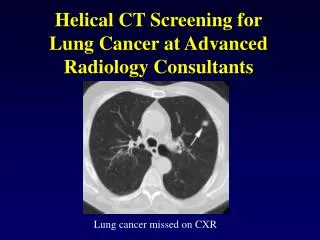
NSCLC: DiagnosisAnd Staging • Chest x-ray • CT scan chest • Distant metastasis evaluation • Bronchoscopy • Trans thoracic needle biopsy • Mediastinoscopy • VATS 30
Surgical ManagementOf Stage 1 And 2 • Wedge resection vs lobectomy • Node sampling N1 and N2 • Refer for adjuvant trials: evaluation of chemotherapy for early stage • Appropriate surveillance 32
Superior Sulcus Tumors • Arm pain • Arm parathesias • Shoulder pain • Horner’s syndrome 33
NSCLC Induction Therapy:Stage IIIA • Surgical staging • Chemo or Radiation/chemo • Evaluate for distant disease • Nutrition • Pulmonary rehab 36
Induction Therapy • Radiation alone • Chemotherapy alone • Radiation and chemotherapy: simultaneous vs sequential • Radiation, and / or chemotherapy with PDT • Pulmonary rehabilitation 37
Pulmonary Resection InThe High Risk Patient • FEV 1 < 0.8 • Hypoxemia • Hypercarbia • Steroid dependent • Elderly • Previous pulmonary resection 43
Pulmonary Rehabilitation • Prepare patient for resection • Decrease hospital stay • Enhance recovery • Promote sense of well being • Minimize impact of chronic illness 44