Download
1 / 59
680 likes | 1.97k Vues
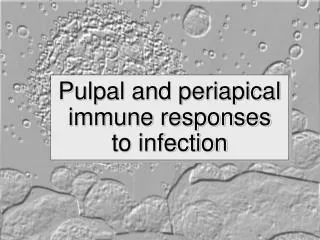
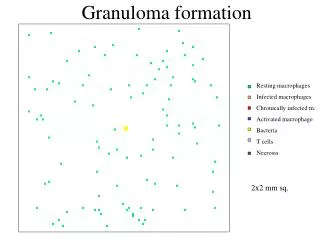
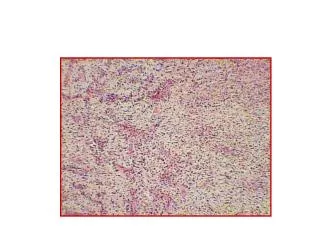
Periapical Granuloma. -Granulation tissue (fibrovascular) -Mononuclear inflammatory cell infiltrate -“chronic inflammation”. Chronic inflammatory reaction in response to a pulpal infection with bacteria. All we can see here are tiny blue dots sprinkled across the entire tissue section.

E N D
Periapical Granuloma • -Granulation tissue (fibrovascular) • -Mononuclear inflammatory cell infiltrate • -“chronic inflammation” Chronic inflammatory reaction in response to a pulpal infection with bacteria. All we can see here are tiny blue dots sprinkled across the entire tissue section. As we shall see next, These are blood leukocytes that have migrated out of vessels into tissue to form what is known as an inflammatory cell infiltrate.
Periapical Granuloma • -Granulation tissue (fibrovascular) • -Mononuclear inflammatory cell infiltrate • -“chronic inflammation” Here we can see some small vessels (arrow) and only faint, immature collagen in the background (pink). The dots sprinkled all around are leukocytes; at this magnification, we can’t definitively identify what types of whites cells they are.
Periapical Granuloma • -Granulation tissue (fibrovascular) • -Mononuclear inflammatory cell infiltrate • -“chronic inflammation” The red arrows point to small round blue nuclei and represent lymphocytes. The blue arrows designate plasmacells; you can see an eccentricnucleous with a purple cytoplasm. Elsewhere in this view, capillaries are present, eosinophilic (pink) collagen is in the background and some of the more spindle shaped cells are fibroblasts.
PA Gran, Subacute Inflammation Notice that the inflammatory cell infiltrate is somewhat different. The background granulation tissue (fibrovascular element) remains unchanged. In this photomicrograph one can identify: macrophages (yellow arrow) plasma cells (blue) neutrophils or PMNs (green) This combination is referred to as subacute inflammation (mononuclear cells and granulocytes). What controls this response? The type of micro-organism does. Certain microbes stimulate an acute response, others a chronic one and yet others, a subacute inflammatory response.
Parulis, acute inflammation This is a biopsy from a draining fistula or parulis associated with an abscessed tooth. At this relatively low magnification one can see a virtural sea of leukocytes and numerous capillaries (red arrows). The granulation tissue here shows no collagen fibers…..only vessels.
Abscess/Parulis This higher magnification discloses a few vessels, some mononuclear cells (very few) and mostly sheets of neutrophiles or PMNs. This is what is termed acute inflammation and when localized under the gingiva it is a submucosal abscess or parulis. In such an instance, the pyogenic bacteria coming out of the necrotic pulp have invaded through bone and out the cortex.
Apical Periodontal Cyst, low In some endodontic infections, not only is there an inflammatory response, but the Rests of Malassez in the apical PDL are stimulated by inflammatory cytokines and growth factors secreted by leukocytes to proliforate. As these epithelial cells increase in size, they become necrotic in the center to create a stratified squamous epithelial lined cavity or cyst. In this low power photomicrograph, the root tips are evident at the top of the view and below is a collapsed cavity. At this power one cannot see the epithelial lining
Periapical Cyst, Medium In this view, one sees the root surface on the right (we cannot actually see the necrotic root canal in this section) To the left is an epithelial lining that still shows proliferation with cords and strands of anastomosing cells. Interposed between the cyst and the root is fibrous connective tissue, a tissue that matured from preexisting granulation tissue. Adjacent to the cyst lining are numerous leukocytes.
APC, Thin Wall This photomicrograph is a low power view of a large apical cyst where one can observe the distended cyst wall, epithelial lining and a lumen filled with amorphous eosinophilic (pink) material that represents the cyst contents of proteinaceous coagulated fluid.
Inflammation in Wall This is a higher magnification of the previous image showing the stratified squamous lining on the left, fibrous connective tissue wall in the center, and on the outer edge is an inflammatory cell infiltrate represented by mononuclear leukocytes, mostly lymphocytes (Chronic inflammation).
Cholesterol Cleft, Multinucleated Giant Cells • In some apical inflammatory lesions, and for reasons not understood, cholesterol accumulates in the fibrous and granulations tissues. • The cholesterol crystallizes into “surf-board” shaped clear cavities. • They are clear because the processing of the tissues for histology uses lipid solvents so all we see are ghosts of the material. • Cholesterol out in the tissues acts as a foreign body and one then sees fused macrophages or multinucleated foreign body type giant cells stretched around the clefts in the process of attempted (in vain we think) phagocytosis.
Pyogenic Granuloma, low mag Now we will take a look at inflammation out in the soft tissues of the gingiva and periodontium. When food particles, popcorn kernals or perhaps even calculus become entrapped in the gingival sulcus, they act as an irritant and stimulate an overzealous proliferation of granulation tissue accompanied by inflammation. This low power photomicrograph was obtained from a gingival mass arising in the interdental papilla. There is an epithelial layer over the top and the mass is composed of granulation tissue.
Pyogenic Granuloma, medium In this medium power view, we can see an epithelial layer on the left and on the right, the mucosal epithelium is lost. This is referred to as ulceration and the surface is represented by a fibrin clot with entrapped neutrophils. The mass is represented by numerous proliferating blood vessels with intervening loose fibrous tissue - an excellent example of very vascular granulation tissue. Leukocytes are distributed throughout.
Pyogenic Granuloma, high This high magnification shows the dilated vascular channels lined by endothelial cells and interposed loose fibrous tissue infiltrated with neutrophils. The term “pyogenic” implies an infectious etiology. It is not. The pyogenic granuloma is a reactive proliferation; reacting to irritation, not infection. This then is an example of the host inflammatory response forming in response to injury.
Mucous Escape Reaction This low power view of a mucocele shows a layer of surface epithelium and an underlying cystic mass filled with purple fluid (mucin). Minor salivary gland lobules are evident on the lateroinferior margin. The mucocele forms as a consequence of ductal severage with escape of secreted mucins into the surrounding connective tissues.
Mucocele Wall When the mucous escapes, it pools and is walled off by granulation tissue. In this medium power view, one can observe the mucin on the top, granulation tissue with underlying dense collagenous tissue in the center and minor salivary glands along the bottom.
Phagocytosis of Mucin At the interface between the granulation tissue wall and the pooled mucin, macrophages can be seen, attempting to phagocytize the mucin. Their nuclei are round and they have a significant amount of pink cytoplasm that has a bubbly or foamy appearance owing to the mucins that have been ingested by these cells
Inflammatory Fibrous HyperplasiaDenture Associated This low magnification specimen shows a lobulated mass represented by a partial covering with epithelium and a massive proliferation of fibrous tissue below. Collections of minor salivary tissue were included in the biopsy.
Inflammatory Fibrous Hyperplasia This low magnification specimen shows a lobulated mass represented by a partial covering with epithelium and a massive proliferation of fibrous tissue below. Collections of minor salivary tissue were included in the biopsy.
Epithelial and Fibrous Hyperplasia At medium power, it can be seen that the surface epithelium is thickened or hyperplastic, a response to trauma from the denture flange. Below is dense mature collagenous connective tissue. This connective tissue appears relatively normal and is traversed by capillaries. Under the epithelium are a few scattered inflammatory cells.
Chronic Sclerosing Sialadenitis The salivary tissues deep in the specimen have also been traumatized and their secretions have been blocked leading to degeneration of the acini. As the acini disappear from apoptosis and necrosis (forms of cell death), inflammatory cells infiltrate and phagocytize the necrotic cells. This is inflammation in response to injury.
Chronic Sclerosing Sialadenitis In this higher magnification, one can see very few remaining acini, although the ducts are more resistant to the trauma and the effects of obstruction. Ductal structures remain in the absence of acini. The normal tissues are then replaced by mononuclear inflammatory cells and the granulation tissue matures into dense fibrous scar-like tissue. Sclerosis means fibrosis or scar formation.