Ref 0282
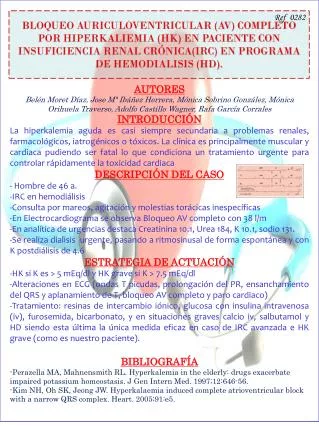
Ref 0282. BLOQUEO AURICULOVENTRICULAR (AV) COMPLETO POR HIPERKALIEMIA (HK) EN PACIENTE CON INSUFICIENCIA RENAL CRÓNICA(IRC) EN PROGRAMA DE HEMODIALISIS (HD). AUTORES

Ref 0282
E N D
Presentation Transcript
Ref 0282 BLOQUEO AURICULOVENTRICULAR (AV) COMPLETO POR HIPERKALIEMIA (HK) EN PACIENTE CON INSUFICIENCIA RENAL CRÓNICA(IRC) EN PROGRAMA DE HEMODIALISIS (HD). AUTORES Belén Moret Díaz, Jose Mª Ibáñez Herrera, Mónica Sobrino González, Mónica Orihuela Traverso, Adolfo Castillo Wagner, Rafa García Corrales INTRODUCCIÓN • La hiperkalemia aguda es casi siempre secundaria a problemas renales, farmacológicos, iatrogénicos o tóxicos. La clínica es principalmente muscular y cardiaca pudiendo ser fatal lo que condiciona un tratamiento urgente para controlar rápidamente la toxicidad cardiaca • DESCRIPCIÓN DEL CASO • - Hombre de 46 a. • IRC en hemodiálisis • Consulta por mareos, agitación y molestias torácicas inespecíficas • En Electrocardiograma se observa Bloqueo AV completo con 38 l/m • En analítica de urgencias destaca Creatinina10.1, Urea 184, K 10.1, sodio 131. • Se realiza dialisis urgente, pasando a ritmosinusal de forma espontánea y con K postdiálisis de 4.6 • ESTRATEGIA DE ACTUACIÓN • HK si K es > 5 mEq/dl y HK grave si K > 7.5 mEq/dl • Alteraciones en ECG (ondas T picudas, prolongación del PR, ensanchamiento del QRS y aplanamiento de T, bloqueo AV completo y paro cardiaco) • Tratamiento: resinas de intercambio iónico, glucosa con insulina intravenosa (iv), furosemida, bicarbonato, y en situaciones graves calcio iv, salbutamol y HD siendo esta última la única medida eficaz en caso de IRC avanzada e HK grave (como es nuestro paciente). • BIBLIOGRAFÍA • Perazella MA, Mahnensmith RL. Hyperkalemia in theelderly: drugsexacerbateimpairedpotassium homeostasis. J Gen InternMed. 1997;12:646-56. • Kim NH, Oh SK, Jeong JW. Hyperkalaemiainduced complete atrioventricular block with a narrow QRS complex. Heart. 2005;91:e5.