Varicose Veins
Varicose Veins. BY PROF . MOHAMED EL GHARBAWI e-mail : elgharma2@yahoo.com Web Site : www.dr-elgharbawi.com. By end you should know Varicose veins Venous insufficiency Venous ulceration. Varicose Veins. Definition : Dilatation, elongation & tortuosity of

Varicose Veins
E N D
Presentation Transcript
Varicose Veins BY PROF. MOHAMED EL GHARBAWI e-mail: elgharma2@yahoo.com WebSite: www.dr-elgharbawi.com
By end you should know Varicose veins Venous insufficiency Venous ulceration
Varicose Veins Definition: Dilatation, elongation & tortuosity of superficial venous system ( In Subcutaneous tissue, not supported) of the lower Limb. NB. Never in Deep venous system ( it is well supported by muscles& fascia)
VARICOSE VEINS ETIOLOGY (II)Primary varicose vein: ‘more common’: The Great saphenous and/or lesser saphenous veins will be dilated , elongated and tortuous with no evident cause or disease. MAY BE DUE TO: 1. Congenital structural weaknesses in vein wall (due to multiple gene familial inheritance) . This is supported by co-incidence of other mesodermal defect disease e.g. hernias, varicocele, piles and ptosis of viscera. 2. Congenital valves incompetence : 9% of people above the age of 45 have incompetence at the saphenofemoral or saphenopopliteal junctions while varicose veins are present in 6%.
VARICOSE VEINS RISK FACTORS RISK FACTORS FOR PRIMARY VARICOSE VEINS: a. F > M (repeated pregnancies). b. Tall & Overweight persons c. Long standing Venous stagnation with subsequent dilatation So, V.V. is common in barbers and surgeons.
VARICOSE VEINS ETIOLOGY • 2ry varicose vein : Secondary to: a. Deep venous thrombosis "Post- phlebitic leg“ (due to obstruction of deep veins). b. Pelvic, abdominal or upper femoral tumors with pressure on the veins, hindering venous flow. c. Arterio - venous fistula (Congenital or acquired). d. Congenital abnormalities (Klippe l- Trenaunay- Weber syndrome and Valvular agenesis)
VARICOSE VEINS COMPLICATIONS 1. Thrombosis: Slow circulation Thrombophlebitis 2. Pigmentation: Extravasation of stagnant R.B.CS destructed with hemosiderin deposition in tissues Brownish pigmentation of skin with itching. 3.Eczema: itching and pruritus ( tissue irritation by hemosiderin. 4. Bleeding: a. due to injury of V.V. with scratching or minor trauma resulting in severe bleeding. Due to valve incompetence, bleeding is coming directly from the heart while the patient is standing. b. It is easily controlled by elevation of the limb and slight pressure on the bleeding point.
VARICOSE VEINS COMPLICATIONS 5. Edema of Ankle & Foot: a. Increase at the end of the day in 1ry varicose V.V. b. Marked constant edema in 2ry V.V. c. Lymphoedema if 2ry infection of V. ulcer occurred resulting in lymphangitis with Lymphatic obstruction
VARICOSE VEINS COMPLICATIONS 6.Varicose ulcer: (2Theories) a. Stagnation, Extravasation of blood , Hemosiderin irritates the tissue , Itching, Scratching and Ulceration Fibrinogen in tissues change into Fibrin, fibrosis around capillaries leading to Anoxia and Ulceration And 2ry infection. b. Leukocytes trapping theory. Leukocytes are trapped in the tissues initiating a destructive inflammatory process and ulceration. And 2ry infection
VARICOSE VEINS COMPLICATIONS V V ULCER is characterized by: • Site: Above the med. Malleolus in lower 1/3 of leg • Size: variable • Shape: Rounded, Oval, Irregular • Margin: Pigmented (Pathognomonic) • Edge: Sloping • Floor: Infected granulation tissue • Base: Minimal indurations, later fixed to underlying bone • Discharge copious amount of seropurulent discharge • Draining Inguinal L.N. 7 .Malignant change: in long standing varicose ulcer Marjolin’s ulcer
CLINICAL PICTURE HISTORY: 1. Primary VV: Females > Males 2. Secondary VV: H/O a cause e.g. DVT, Penetrating wound Symptoms: 1. Discomfort or dull aching pain in the limb. 2. Cosmetic disfigurement "especially in females". 3. Slight pain in the foot towards the end of the day V. V. or F.F (Flat foot). 4. Swelling around ankle: Primary (mild), 2ry (Severe) 4. Symptoms of complication
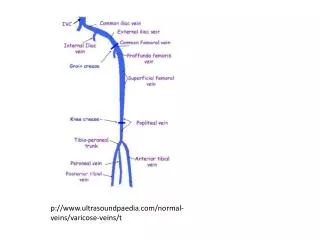
CLINICAL PICTURE GENERAL EXAMINATION: • Other conditions of mesodermal weakness e.g. varicocele, hernias, piles, etc… (1ry V V) • A -V Fistula with hyperdynamic circulation, Abdominal or pelvic mass, etc… (2ry V V) LOCAL EXAMINATION: • Varicose veins appear as tortuous, dilated, elongated bluish veins affecting the well known great and/or small saphenous veins. • Varicose veins may appear as isolated tortious, dilated bluish bunches of veins without saphenous system affection. • V V are soft cystic and compressible swellings • Saphena Varix : Appears as soft cystic bluish compressible swelling at upper part of femoral triangle opposite the upper end of Great saphenous vein. It is due to incompetence of saphenous femoral junction. Coughing lead to thrill and expansile impulse.
CLINICAL PICTURE (A) Is it 1ry or 2ry: 1. Unilateral varicose vein with constant edema and short duration with pigmentations and sometimes ulceration are in favor of diagnosis of 2ry VV. 2. History suggesting D.V.T. or abdominal tumor. 3. Palpation of thrill or accompanying congenital vascular malformation (CVM) 4. Dilated veins in the pubic region usually direct the attention to D.V.T. with dilated veins to bypass high obstruction in the iliac veins.
CLINICAL PICTURE 5. Perthes' test (To evaluate patency of deep v. system): Patient lies down, evacuate veins by elevation of LL. A bandage is applied to the leg from the toes to groin (to obliterate superficial v. system) then ask the patient to do exercise for 20 min. • It is subjective test depends on patient's threshold of pain. • If pain occurs this means that there is obstruction of deep system = 2ry varicose veins. • If no pain but some relieve occurs this means that the deep system is patent = 1ry varicose veins.
CLINICAL PICTURE 6. Modified Perthes' test: Tourniquet is applied immediately below the saphenous opening to occlude drainage of superficial veins. Then, ask the patient to exercise for 5 minutes • If marked engorgement of saphenous system with pain occurs = Obstruction of deep system =2ry V.V. • If No engorgement = Patent deep system = 1ry V.V. • It is an objective test
CLINICAL PICTURE (B) If 1ry where is the level of incompetence? 1. Feeling of thrill while gentle palpation over the site of saphenofemoral junction and asking the patient to coughindicates incompetence at saphenofemoral junction.
CLINICAL PICTURE 2.Schwartz test: While the patient is standing and if the saphenous vein is dilated, put your finger at the lower part of the vein and a finger of the other hand at the upper part of the vein. Normally if you do percussion by the lower finger, you can feel transmitted thrill with the upper one and the reverse does not work due to saphenous vein valves. If you feel transmitted thrill by the lower finger while doing percussion with the upper one this means that there is incompetence of the saphenous vein valves.
CLINICAL PICTURE 3.Trendlenburg test: a. The patient lie supine while elevating his limb and evacuating veins by milking. b. Obstruct the saphenous opening 1.5" below & lat. to pubic tubercle by applying tourniquet just below it. c. Ask the patient to stand. Normally the veins shows slow filling from down upwards. • If there is rapid filling of veins from below. The • incompetence is below the saphenofemoral • valve, • If no filling occurs except after removal of the • finger. The incompetence is at sapheno- femoral • valve
CLINICAL PICTURE 4.Multiple tourniquet test: • After evacuation of engorged veins while patient is supine, Apply 3-4 tourniquet at upper thigh, mid-thigh. • Ask the patient to stand and detect the sites of blow out. 5. 2bandage test: • Apply one bandage from the toe upward to the groin. • Then ask the patient to stand. • Remove the bandage from above while applying another one at the sites of removed bandage and detect the sites of blow out
INVESTIGATIONS 1.Phlebography: Ascending venography can detect the presence of D.V.T and detect patency of deep system. Descending venography (Inject dye into the femoral vein and ask patient to strain and see the condition of perforators and incompetent valves by regurge of the dye into superficial system at site of Blowout site). As mentioned before it can map the varicosities and its origin. Recently its role is declining in comparison to the less invasive duplex scanning.
INVESTIGATIONS 2.Duplex Ultrasonography: Recently it replaces venography and it gives all data needed especially in above and below knee especially in skilled operator hands. It is less invasive and cheaper than phlebography.Can give full data as discussed before a. It can comment on both sapheno -femoral and spheno -popliteal if they are competent or not. Also the degree of incompetence can be evaluated. b. It can detect the sites of incompetent perforators and mark them on the skin to facilitate surgery c. It can detect incompetence of the deep veins and superficial veins.
INVESTIGATIONS 3. Arteriography: It diagnoses A-V fistula with 2ry V V
Differential Diagnosis: of venous ulcer OTHER CAUSES OF LEG ULCERS: 1. Traumatic ulcer: • Spreading type with red margin & increasing size • Callous • Healing ulcer : diminishing in size with surrounding rim of violet skin 2. Infective ulcer: • Non specific: ulcerating carbuncle, ulcerating pyoderma gangrenosum • Specific: • T.B.: It has irregular outline, undermined cyanotic edge & deficient • anemic granulation tissue in the floor. • Syphilis: Chancre in 1ry syphilis, Gummatous Ulcer in tertiary • syphilis: circular outline, punched out edge, indurated base and a • wash leather slough at the floor, ulcer tends to heal and breakdown • again. • Leishmania: superficial spreading ulcer with punched out edge, positive for • leshmania Donovani bodies.
3. Neoplastic: • Rodent ulcer: It has rolled in edge, beaded, slowly growing, floor is red granular and often covered by dry crust or scab, • Epithelioma: it has raised everted edges, indurated base, rapidly growing ,may be fixed to underlying tissue, floor is occupied by malignant fungating tissue, • Ulcerating melanoma 4.Venous Ulcer: as described above. 5.Ischemic ulcer: Undermined edge due to the fact that subcutaneous tissue suffers more from ischemia. 6.Self inflected Ulcer: In reachable site, in patients with hysterical background
Treatment • Varicose vein treatment depends on the patient's complaint and the degree of the disease. • Palliative treatment: • Indications: • 2ry V.V. • Spider varices with normal saphenous system. • Methods: • Removal of the cause or predisposing factor by changing the lifestyle of the patients. They should leave sedentary life, avoid longstanding and reduce their weight. • Wearing elastic stocks during the day time.
II.Injection treatment: • Indications: 1- Early cases of 1ry V.V with competent valves. 2- Residual varices after operation. • Drugs: 1. Sclerovein (polydodecan) 2. Sclerozan (Ethoxysclerol) 3. Na morrhuate 4. Ethanolamine Oleate. • Method: • The patient stand the veins will be engorged. • The needle is introduced to the engorged veins. • Then the patient lies down to evacuate the vein from blood.
• Inject 2 ml of the sclerosing material to destruct the intima of vein and obstruct it. • Apply bandage from the toes level to above the injection level. This bandage should not be removed before one week. • Maximum dose is 6cm at different levels in one setting. • Repeat after 2-3 weeks till all V.V. are obliterated. In most situations it is used for cosmetic disfigurement.
SCLEROTHERAPY Before & After Before & After
FOAM INTRAVASCULAR INJECTION Recently some techniques are described to inject the main saphenous trunk and the incompetent perforators guided by duplex ultrasonography. For this purposes a foam material is prepared using the sclerosing agent by repeated injection of it through narrow nuzzle syringe into another syringe using 3 way connection till it become mixed with air and attain foam character. This technique thought to replace surgery in cases with advanced varicose vein. The foam is lighter than blood so. the limb should be elevated with slight head down to avoid air embolism.
Complications: 1. Extravenous leakage inflammation & abscess. 2. The dye reach deep system D.V.T. 3. Allergic reaction. 4. Permanent pigmentation at sites of injection. III. Surgical treatment: • Indications: 1. Large primary V.V. with incompetent valves. 2. Pain and heaviness of the diseased limb or complication occurs. • Operations: 1. Ligation. 2. Stripping. 3. Laser photocoagulation.
1- LIGATION: (a) Trendlenburg's operation: IndicationIncompetent saphenofemoral valve with healthy saphenous vein valves. Technique Ligation of the saphenous V. in flushing with femoral vein and ligation of its 5 tributaries which are: 1. Superficial epigastric V. 2. Sup. circumflex iliac V. 3. Sup. Ext. Pudendal V. 4. Two unnamed (posteromedial and posterolateral vein). (b) Multiple ligation: Indication when multiple perforators are incompetent despite healthy saphenous systems. Technique Through multiple small incisions exposing the marked sites of incompetent perforators do ligature of the perforator and excision of the involved segment.