Download
1 / 27
270 likes | 570 Vues
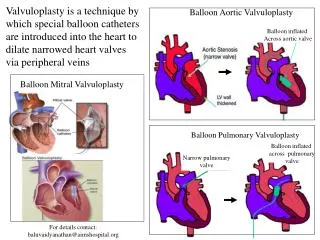
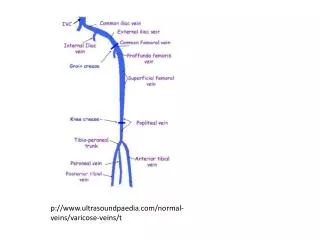
p :// www.ultrasoundpaedia.com /normal -veins/varicose -veins /t . Anatomy.

E N D
Anatomy • The plantar digital veins-rise from the plexuses on the plantar surfaces of the digits -join dorsal digital veins-form 4 metatarsal veins - communicate by perforating veins to form the deep plantar venous arch. • -the medial and lateral plantar veins communicate with the great and small saphenous veins(GSV &SSV) unite behind the medial malleolus to form the posterior tibial(PTV)
The PTVs are paired and run medially in the calf near the tibia accompanied by the PTA and arise via tributaries between the medial malleolus and the Achilles tendon at the ankle. The Peroneal veins are paired -run deeper in the calf parallel to the PTVs through most of the calf adjacent to the fibula The anterior tibialvein(ATV) are the upward continuation of the venae comitantes of the dorsal pedis, they join the Tibioperoneal trunk to form the Popliteal vein The popliteal vein(POPV) –formed by the junction of the ATV and TP trunk at the lower border of the popliteus -ascends through the popliteal fossa and becomes the femoral vein in the adductor canal. Contains 4 valves and commonly dupplicated
The femoral vein (FV)runs upward along with femoral artery(FA) lies lateral to the artery-lies medial at the inguinal ligament-joined by the deep femoral(profundafemoris)towards its termination into the common femoral vein. The deep femoral vein(PF)receives tributaries corresponding to the perforating branches The common femoral Vein (CFV) is joined by the GSV at the junction before it becomes the external Iliac vein The GSV –arises from medial marginal vein of the dorsum of the foot- runs in front of the tibial- malleolus along the medial side of the legs in relation to the saphenous nerve – ends into the CFV 3cm below the inguinal ligament.
The small saphenous vein(SSV) originates from the lateral foot-passes posteriorly lateral to the achilles tendon - centrally along the superficial aspect of the calf between two heads of the gastrocnemius muscle and drains in the POPV. The superficial venous system is a complex web like network of interconnecting veins The foot perforators Ankle perforators (Crokett’s) Calf perforators Knee perforators (Boyd’s) Thigh perforators(Hunter’s/Dodd’s)
Source:http://venacure-evlt.com/endovenous-laser-vein-treatment/procedure/venous-anatomy/
Deep veins and Superficial veins Deep vein thrombosis and Thrombophlebitis Ultrasound of the leg for suspected DVT • EQUIPMENT SELECTION • A 3-9 or 12 MHz linear transducer, a curve –linear transducer can be used for the Iliac veins and for calf veins in obese/large patient • Low velocity range to demonstrate good colour filling of the vessels • Low wall filter and wide sample volume to gain as much information as possible
Scanning Protocol • The leg under examination should be accessed from the groin to the ankle. • Dual imaging is necessary to show one side normal and other side demonstrating compression • B-mode • Transverse section -starting at the inguinal canal-examining the: • Common femoral vein, Greater saphenous junction, femoral and profunda femoral vein, femoral vein proximal, mid and distal into the adductor canal, compressing the veins every 2-3 centimeters. • Colour and spectral Doppler in longitudinal showing the – • Common femoral vein, Greater saphenous junction, • bifurcation of the deep and femoral veins, • femoral vein-proximal, mid and distal
B-mode transverse images of the Popliteal vein, proximal and distal demonstrating compression Longitudinal colour and spectral Doppler of the popliteal vein B-mode transverse images of the posterior tibial and peroneal veins demonstrating compression Longitudinal colour and spectral Doppler images of the posterior tibial and peroneal veins B-mode images of the medial and lateral gastrocnemius, soleal, long and small saphenous veins
Venous dysfunction develops when the venous return is impaired -due to abnormalities from within the deep /superficial veins or a combination of venous obstruction-thrombotic or non thrombotic or from valvular incompetence, which maybe segmental or involving the entire length of the vein Patient’s symptoms-vary-from non obvious-to pain, redness, oedema, dilatation of the superficial veins of the affected leg. Homans sign-pain in the calf with forced dorsiflexion of the foot
Risk factors • Malignancy • Long distance travel(by air or by road without excise) • Pregnancy • Obesity • Post surgery or trauma • Immobilisation • Past history of DVT • Contraceptive pills
Age-increasing age increases the risk of developing DVT. • Coagulation disorders(congenital/acquired) • Septicaemia • Past history of DVT • Hormonal replacement therapy • Stroke • Stacis of blood flow • Smoking.
Criteria for diagnosing thrombosis • Inability to compress the vein • Visible intraluminal clot-fresh echolucent -old increasingly echogenic • Absence of flow in the vein • Diameter of the vein-increases in acute phase-smaller in chronic phase. • Loss of change in diameter in the CFV during valsalva manoeuvre • Minimal augmentation • Increased flow in the superficial veins-they act as collaterals
Pathology • Baker’s cyst(semi-membranosis-gastrocnemialburser)in the medial popliteal fossa • Cellulitis, Lymphoedema, Lymphangitis • Superficial venous thrombosis of varices and of the great and small saphenous veins • Calf muscle tear • Deep vein thrombosis • Pulmonary embolism
Sample images showing normal compressible deep veins and thrombus in the short saphenous vein(thrombophlebiti the and sapheno-poplitealjunction propagating into the deep vein(popliteal). Thrombus also seen in superficial varicose veins Veins. Diagnosis deep vein thrombosis with thrombophlebitis.
References Hamper, M.U., M.R. DeJong, and L.M. Scoutt. 2007. Ultrasound evaluation of the lower extremity veins. Radiologic Clinics of North America 45: 525-545. • Kupinski, A.M. 2013. Diagnostic medical sonography. The vascular system. Philadelphia: J.K. Stegman3 • Myers, K.A and A. Clough. 2004. Making sense of vascular ultrasound a hands on guide. London: Arnold • Zwiebel, W.J., and J. Pellerito. 2005. Introduction to Vascular Ultrasound. 5th ed. Philadelphia: W.B. Sanders