Download
1 / 52
550 likes | 1.36k Vues
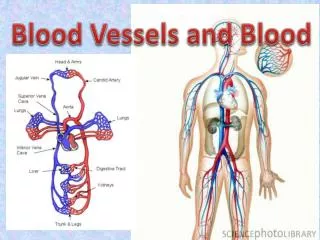
Blood, Blood Vessels & Circulation. Cardiovascular System. Blood vessels: Types. A. Arteries -carry oxygenated blood (most of the time) away from the heart -thicker than veins -three layers: inner endothelium middle smooth muscle outer connective tissue

E N D
Blood, Blood Vessels & Circulation
Cardiovascular System Blood vessels: Types A. Arteries -carry oxygenated blood (most of the time) away from the heart -thicker than veins -three layers: inner endothelium middle smooth muscle outer connective tissue -arteriole = small artery B. Veins -carry deoxygenated blood (most of the time) – toward the heart -same three layers as arteries (less SM and connective tissue) -thinner and more expansive than arteries -contain valves - to help the flow of blood back to heart -small vein = venule C. Capillaries -site of gas exchange with tissues -connect arterioles and venules -network of microscopic vessels (one cell thick) = capillary bed -site of exchange: gases, nutrients, wastes -can be closed off when not needed
Arteries • Tunica interna (intima) • simple squamous epithelium known as endothelium • basement membrane • internal elastic lamina • Tunica media • circular smooth muscle & elastic fibers • smooth muscle is innervated by sympathetic nervous system • decrease in stimulation or presence of certain chemicals causes vasodilation • increases diameter of vessel • nitric oxide, K+, H+ and lactic acid cause vasodilation • increase in stimulation causes muscle contraction or vasoconstriction • decreases diameter of vessel • Tunica externa • elastic & collagen fibers
Elastic Arteries • Largest-diameter arteries have lot of elastic fibers in tunica media • Help propel blood onward despite ventricular relaxation (stretch and recoil -- pressure reservoir) Muscular Arteries • Medium-sized arteries with more muscle than elastic fibers in tunica media • Capable of greater vasoconstriction and vasodilation to adjust rate of flow • walls are relatively thick • called distributing arteries because they direct blood flow
Blood flow & Pressure gradients • blood flow is fastest in the arteries • slows within arterioles • slowest rate in capillaries - allows forexchange • blood flow becomes faster when vessels merge to form veins • flow rate through a vessel is proportional to the pressure gradient and inversely proportional to the vascular resistance (diameter) • F = ΔP/R • F = flow rate • ΔP = pressure gradient • R = resistance • ΔP is the pressure gradient = difference in P between the beginning and end of a vessel • this is what determines flow rate – NOT the absolute pressure! • resistance changes as the radius changes • R increases as r decreases – F will decrease (if P stays the same) • R decreases as r increases – F will increase (if P stays the same) • this relationship applies to non-viscous fluids
Blood flow & Pressure gradients • frictional losses (resistance) causes a drop in P as the blood travels through a section of vessel • caused by friction between the moving fluid and the stationary wall • if pressure gradient is unchanged – then increasing R will inhibit blood flow and decrease F • R depends on three factors • 1. blood viscosity (η) - # of circulating RBCs • 2. vessel length (L) • 3. vessel radius (r) – major determinant of R • R = 1/r4 • Pouiseuille’s Law • Flow rate = η ΔP r4 8 ηL
Blood Pressure • Pressure exerted by blood on walls of a vessel • depends on the volume of blood within the vessel and the distensibility of the vessel • caused by contraction of the ventricles • highest in aorta • 120 mm Hg during systole & 80during diastole • difference between systole and diastole – pulse pressure • the volume of blood entering an artery is not the same as the volume leaving it • during ventricular systole – the SV leaving the artery is 1/3 of that entering the artery • because the artery will distend with increasing volumes • during diastole – the recoil of the vessel drives the exit of the blood • If heart rate increases cardiac output, BP rises • mean arterial pressure – average pressure driving blood forward into the tissues throughout the cardiac cycle • at resting heart rate – about 2/3 of the cardiac cycle is spent in diastole • MAP falls steadily insystemic circulation with distance from left ventricle • 35 mm Hg entering the capillaries • 0 mm Hg entering the right atrium
F = ΔP/R applies to the entire circulatory system in addition to a single vessel • F = cardiac output • ΔP = MAP (ΔP = difference in pressure at the beginning of the systemic circulation and the end of the systemic circulation) • MAP as the blood leaves the left ventricle (93 mm Hg) – the MAP as the blood enters the right atrium (0 mm Hg) • R = total peripheral resistance = total resistance offered by all systemic peripheral vessels • influenced by sympathetic nervous activity • rearrange the equation - ΔP = F X R • OR MAP = CO X total peripheral resistance
1 – CO and total peripheral resistance • 2 – CO depends on heart rate and SV • 3 & 4– heart rate depends on balance between the parasymp and symp divisions of the ANS • 5 – SV increases in response to symp activation (extrinsic control) • 6 – SV also increases with increasing venous return (instrinsic control) • 7- 10 – venous return is increased by symp induced vasoconstriction (7), skeletal muscle pump (8), respiratory pump (9) and cardiac suction (10) • 11 – 13 – venous return is also influenced by how much blood returns to the heart (11), actual blood volume (balance between passive bulk-flow fluid exchange between plasma and ECF (12), water and salt balance (13) and hormonal control (14)
15 & 16 – MAP is also determined by radius of the vessel (15) and the number of RBCs (16) • 17 - 20– arteriole radius can be controlled by metabolic factors which control blood need (17) - which leads to vasodilation (18) ALSO by sympathetic activity (19) which can cause vasocontriction (20) OR hormonally (20)
Arterioles • major resistance vessels in the vascular tree • radius is small enough to offer resistance to flow • high arteriolar resistance causes a marked drop in the MAP as blood flows through these vessels • MAP arteriole entrance = 93 mm Hg • MAP arteriole exit = 37 mm Hg • establishes a pressure differential that encourages flow of blood into the capillary beds within the tissue • resistance also converts the pulsatile nature of systolic-diastolic pressure to nonpulsatile pressure within the capillaries • radius of the arteriole can be adjusted to • 1. variable distribute cardiac output among the organs • 2. help regulate arterial blood pressure
Arterioles and Arteriolar resistance • vasoconstriction and vasodilation • presence of a thick layer of smooth muscle • sensitive to many systemic, local factors + neurogenic stimulation • vascular tone • arterioles normally exhibit a state of slight constriction = vascular tone • helps establish a baseline of arteriolar resistance • tonic activity makes it possible to either vasoconstrict or vasodilate • two facets are responsible • 1. myogenic activity of smooth muscle layer • smooth muscle layer is responsive to neural or hormonal influences – self-induced contractile activity • 2. continuous release of NE by sympathetic fibers of the ANS
we have evolved mechanisms to ensure that blood flow into an organ falls within a specific range = autoregulation • not all organs autoregulate at the same level – brain has poor autoregulatory mechanisms • autoregulation can be performed by the tissues (intrinsically) and/or by the nervous system (extrinsically)
Chemical influences and arteriole radius = local metabolic changes • most important local chemical influences on arteriolar smooth muscle are local changes in metabolism within that organ • local metabolic changes can affect the diameter of an arteriole without neural influence • active hyperemia = local arteriolar vasodilation that increases blood flow into an organ • local metabolic factors • decreased/increased oxygen = vasodilation/vasoconstriction • increase carbon dioxide = vasodilation • increased carbonic acid= vasodilation • increased K+ - repeated APs that outpace the Na/K pump’s ability to correct ionic changes = vasodilation • increased osmolarity – concentration of solutes accumulates in actively metabolic cells = vasodilation • adenosine release – cardiac muscle – release in response to increased metabolic activity = vasodilation • prostaglandin release = vasodilation • relative concentration of these factors can determine the state of arteriolar muscle tone
Vasoactive Mediators • these local chemical changes do not act directly on smooth muscle but act on the endothelial cells • ECs – simple squamous epithelial cells • ECs then release chemical factors called vasoactive mediators • e.g. endothelin = vasoconstriction • e.g. nitric oxide = vasodilation by relaxing arteriolar smooth muscle • inhibits entrance of calcium into the smooth muscle which inhibits the opening of the foot proteins on the sarcoplasmic reticulum • ECs have multiple roles
Histamine • NOT released by metabolic changes • NOT produce by endothelial cells • released upon pathology • released by connective tissue cells within the organ or by circulating white blood cells (mast cells, basophils) • usually released in response to organ damage • causes vasodilation to increase blood flow and speed healing
Local Physical factors • application of heat or cold • heat causes localized arteriolar vasodilation • increases blood flow • cold – counteracts histamine-induced swelling by inducing vasoconstriction • shear stress • blood flowing over the endothelial lining creates friction = shear stress • increase in shear stress can cause increased release of NO – promotes vasodilation • increased blood flow now reduces shear stress • myogenic response to stretch • increased MAP drives more blood into the arteriole which pushes out against the vessel wall = passive stretch • extent of passive stretch is related to the volume of blood through the vessel tone • this increased tone acts to resist the passive stretch • in other words- arteriolar smooth muscle responds to passive stretch by increasing its tone through vasoconstriction • arterial occlusion can block blood flow and reduce this stretch • arterioles will dilate in response • reactive hyperemia
Extrinsic control of arteriolar diameter • includes both neural and hormonal control • sympathetic division innervates arteriolar smooth muscle everywhere except the brain • NO parasympathetic innervation of arteriolar smooth muscle! (exception – ciltoris and penis) • sympathetic activity contributes to arteriolar vascular tone • increased sympathetic activity induces vasodilation of arterioles in heart and skeletal muscle– drops arteriolar resistance and changes MAP
the extent of total peripheral resistance influences the MAP dramatically • MAP = CO X TPR • if you increase R (by decreasing vessel diameter) you increase MAP • in other words you have to increase MAP to maintain flow rate • WHY? why increase the driving force of blood into an organ by increasing pressure (MAP) but decrease blood flow into the organ by increasing R (decreasing vessel diameter)????? • the sympathetic nervous system essentially maintains an appropriate driving pressure to each organ but the organ itself controls the amount of blood that actually enters it. • sympathetic control over arteriolar vascular tone constricts most vessels to ensure adequate MAP throughout the systemic circuit • therefore the organ can override the sympathetic control by local arteriolar control mechanisms and ensures adequate MAP • analogy = water pressure in pipes
HORMONAL CONTROL OF ARTERIOLAR DIAMETER: • angiotensin II – converted from angiotensin I by the enzyme ACE (produced in the lungs) • regulates body’s salt balance • powerful vasoconstrictor • vasopressin (ADH) – released from the posterior pituitary in response to changes in water volume • drop in water content, release of vasopressin, decreased urine volume, increased water retention • also a vasoconstrictor
Epinephrine and Norepinephrine; can be released from either the adrenal medulla (sympathetic activity) or from neurons (sympathetic or parasympathetic activity) • release of epinephrine and NE from the adrenal medulla reinforces sympathetic reflex activity • Ep and NE can cause vasocontriction or vasodilation!!! depends on receptor and its location • Ep and NE can also bind to a1-adrenergic receptors on arteriolar smooth muscle to increase vasoconstriction • cerebral arterioles do NOT have a1-adrenergic receptors !!! • influence entirely by local physical and chemical changes (intrinsic changes) - b2 receptors are located on arteriolar smooth muscle in cardiac and skeletal muscles - vasodilation • Ep is more abundant – has more affinity for the b2-adrenergic receptors which are expressed in large amounts on arteriolar smooth muscle in skeletal and cardiac muscle
Continuous capillaries • skeletal & smooth, connective tissue and lungs • Fenestrated capillaries • plasma membranes have many holes • kidneys, small intestine, choroid plexuses, ciliary process & endocrine glands • Sinusoids • very large fenestrations • incomplete basement membrane • liver, bone marrow, spleen, anterior pituitary, & parathyroid gland Capillaries • Microscopic vessels that connect arterioles to venules • Found near every cell in the body but more extensive in highly active tissue (muscles, liver, kidneys & brain) • entire capillary bed fills with blood when tissue is active • lacking in epithelia, cornea and lens of eye & cartilage • Function is exchange of nutrients & wastes between blood and tissue fluid • Structure is single layer of simple squamous epithelium and its basement membrane
capillaries are not open under resting conditions in most tissues • prevents the flow of blood through the capillary bed • capillaries branch from a metarteriole or directly from an arteriole • metarteriole acts like a thoroughfare connecting a larger arteriole and a venule • these MAs are surrounded by spiralling smooth muscle cells – form a precapillary sphincter • the sphincters are not innervated by the nervous system by still possess a high degree of myogenic tone to contract in response to chemical factors released by the tissue • the more metabolically active the tissue, the greater the number of capillaries • e.g. muscle • only 10% of the capillaries are open in resting muscle • as the muscle increases its activity – local chemical factors change and the precapillary sphincters open to allow more blood flow
ECs fit together like a jigsaw puzzle with considerable gaps in between the cells = pores • sizes vary from capillary to capillary • brain capillaries have EC cells held together by tight junctions – no pores • most tissue capillaries allow the passage of small water-soluble substances but don’t allow the passage of larger non lipid-soluble materials • this transport may actually be regulated by the capillary itself • in the liver, the capillary walls have larger pores to allow the passage of proteins
Interstitial Fluid or ECF • passive intermediary between blood and cells – not a direct exchange between the blood and the ICF of cells • only 20% of the ECF circulates as plasma • the remaining 80% is interstitial fluid • exchange between the inside of the cell and the interstitial fluid (across the plasma membrane) is passive or active – depending on the cell and the solute being moved • BUT exchange between the interstitial fluid and the capillary wall is primarily PASSIVE • there is a limited amount of active transport – vesicular transport • because the gaps in a capillary wall are quite large, the interstitial fluid and the composition of the blood are essentially the same • two ways to exchange materials between the blood and interstitial fluid • 1. diffusion • 2. bulk-transport
Diffusion • diffusion is promoted by several factors: • 1. short distance of travel • 1. thinness of the capillary wall – 1 um in thickness (simple squamous epithelium + basement membrane) • 2. narrowness of the capillary – thinner than the RBC so the cells must pass through one at a time • 3. proximity to cells – every cell is approximately 0.01cm from a capillary • 2. total surface area – 10 to 40 billion capillaries • produces a tremendous surface area for exchange = 600m2 • SA of the capillaries is 1300 times greater than the SA of the aorta • 3. velocity through the capillary • slowest velocity is found in the capillaries • called “velocity of flow” rather than “flow rate” • NOT a measure of volume over time (F) • analogy – river – lake – river • flow rate (volume of water) flowing past any point along the river = that of the lake • however, the speed of the water flowing is slower in the lake
Bulk-flow • a volume of protein-free plasma filters out of the capillary and mixes with the surrounding interstitial fluid and then is reabsorbed = bulk flow • the various components are moved in bulk in contrast to the movement of individual components as seen in diffusion • when pressure inside the capillary exceeds that of the pressure in the interstitial fluid – fluid is pushed out through the pores in the capillary wall = ultrafiltration • most of the plasma proteins are still retained in the blood’s plasma because of the size of these proteins and the size of the pores • with the fluid comes the movement of multiple other components • when inward driving pressure exceeds the outward – net inward movement of fluid and fluid components = reabsorption • ultrafiltration and reabsorption are collectively known as bulk flow • does NOT play a role in the exchange of individual solutes • does play a role in regulating the distribution of ECF between the circulating plasma and interstitial fluid
Bulk Flow • (Pc + πIF) – (πP + PIF) = outward pressure – inward pressure • major factors are Pc and πP
1. Pc = capillary blood pressure • fluid or hydrostatic pressure exerted on the inside of the capillary wall by blood • tends to force fluid OUT of the capillaries into the interstitial fluid • 2. πP = plasma-colloid osmotic pressure (oncotic pressure) • force caused by colloidal dispersion of plasma proteins- encourages inward movement of fluid into the capillary • because plasma proteins cannot leave the plasma – there is a protein concentration difference and a water concentration difference between the blood and interstitial fluid (higher water in the interstitial fluid, lower protein) • this exerts an osmotic pressure difference than promotes the movement of water OUT of the interstitial fluid to the blood plasma to decrease the rising osmotic pressure in the blood
3. PIF = interstitial fluid hydrostatic pressure • fluid pressure exerted on the outside of the capillary wall by interstitial fluid • tends to force fluid into the capillaries and into the blood plasma • 4. πIF = interstitial fluid-colloid osmotic pressure • does not normally contribute significantly to bulk flow • promotes the osmotic movement of water out of the blood and into the fluid to decrease the rising osmotic pressure in the tissues
Net exchange of fluid across capillaries • Net exchange pressure = (Pc + πIF) – (πP + PIF) = outward pressure – inward pressure • two pressures forcing fluid out of the plasma are capillary blood pressure and interstitial fluid-colloid pressure • two pressures forcing fluid into the plasma are plasma-colloid osmotic pressure and interstitial fluid hydrostatic pressure • the imbalance between the forces produces a net exchange of fluid at a given point along the capillary wall • as the blood enters the capillary – outward forces exceed that of inward and fluid is forced out into the interstitial fluid (no protein movement!) – ultrafiltration forces result • as the blood moves through the capillary – pressure drops • at the venular end the inward pressure now exceeds the outward pressure and reabsorption will take place • so the amount of fluid moving out of the blood drops as the blood travels through the capillary region and progressively increasing amounts of fluid re-enter the blood as the blood reaches the venular end of the capillary
Lymph • even under normal circumstances – more fluid is filtered from the blood plasma into the interstitial fluid than is reabsorbed back into the blood plasma • excess fluid = lymph • this excess fluid is directed into a series of vessels that are similar in structure and composition to veins – lymphatic vessels • one-way system of vessels that leads back to the circulatory system via the right lymphatic duct and the thoracic duct
Regulation of BP • regulation of mean arterial pressure by the body • the body actually monitors: • MAP = cardiac output x total peripheral resistance • BP is measured constantly by baroreceptors • changes in pressure within blood vessels • two major BRs: carotid sinus & aortic arch baroreceptors (mechanoreceptors) • respond to changes in pulse pressure through the common carotid artery and aorta • provide information about mean arterial pressure by generating action potentials in response to being stretched • role of cardiovascular center in the medulla • help regulate heart rate & stroke volume • integrating center for information sent by the carotid and aortic BRs • divided into two centers: vasomotor & cardiac centers (cardioacceletory, cardioinhibitory divisions) • alters the ratio between sympathetic and parasympathetic activity to the heart and BVs • specific neurons regulate blood vessel diameter - sympathetic vasomotor nerves • signals sent out through vagus & cardiac accelerator nerves - changes heart rate
Higher brain centers such as cerebral cortex, limbic system & hypothalamus also play a role • anticipation of competition • increase in body temperature • Hypothalamus • osmoreceptors control salt and water balance and therefore long-term regulation of BP • cerebral cortex-hypothalamus preprograming – fight or flight responses, sexual orgasm, blushing • control over cutaneous arterioles for temperature regulation takes control over the cardiovascular center’s control over these vessels for regulation BP • therefore BP can fall dramatically as arteries dilate to allow cooling • Proprioceptors • input during physical activity • Chemoreceptors • monitor concentration of chemicals in the blood (O2, CO2 and H+ions) • also located in the carotid and aortic arteries • increase respiratory activity to bring in more O2 or blow off more CO2 • also increase BP by sending excitatory impulses to the cardiovascular center
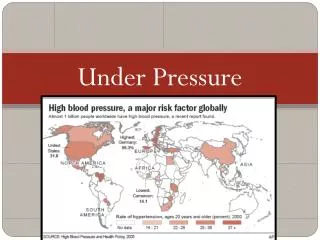
Medical application: Hypertension • primary and secondary hypertension • secondary hypertension: occurs secondary to another disorder • 1. renal hypertension – artherosclerotic lesions in the renal artery or other disruptions to the flow of blood into the kidney • kidney responds by releasing renin – initiates the renin-angiotensin II-aldosterone pathway • increased salt and water retention • increases blood volume – increases BP • angiotensin II is also a powerful vasoconstrictor • 2. endocrine hypertension • tumors of the adrenal glands can cause excessive secretion of epinephrine and NE – increase cardiac output • 3. neurogenic hypertension • erroneous neural control • primary hypertension: caused by a variety of reasons • defects in salt management by kidneys – accumulation of salt and water in blood • excessive salt intake – salt osmotically retains water and expands plasma volume • diets low in fruits, vegetables and dairy products – low K+ and Ca+ • K+ from fruits and vegetables may relax artery walls • role of calcium is still unclear • defective Na/K pump activity – changes electrical excitability of cardiac muscle cells and smooth muscle cells – higher BP • Na/K pumps are also critical to salt managment • variations in the gene that codes for angiotensinogen • part of the hormonal path that synthesizes angiotensin II • defects in this path can promote salt and water retention in the blood • endogenous digitalis-like substances • act similarly to digitalis to increase cardiac contractive strength and therefore cardiac output • also increases vasoconstriction of arteries • abnormalities in NO, endothelin or other vasoactive chemicals • NO = vasodilator • shortage in NO has been seen in some hypertensive patients • endothelin = locally acting vasocontrictor (genetic problems) • excessive vasopressin (somatostatin) – vasocontriction and water retention
Evaluating Circulation • Pulse is a pressure wave • alternate expansion & recoil of elastic artery after each systole of the left ventricle • pulse rate is normally between 70-80 beats/min • tachycardia is rate over 100 beats/min/bradycardia under 60 • Measuring blood pressure with sphygmomanometer • Korotkoff sounds are heard while taking pressure • systolic blood pressure from ventricular contraction • diastolic blood pressure during ventricular contraction • provides information about systemic vascular resistance • pulse pressure is difference between systolic & diastolic • normal ratio is 3:2:1 -- systolic/diastolic/pulse pressure
Veins • Proportionally thinner walls than same diameter artery • tunica media less muscle – little inherent myogenic tone • lack external elastic lamina • tunica externa has more collagen than elastic fibers • strong and stretchy but possess poor elastic recoil • Still adaptable to variationsin volume & pressure • Valves are thin folds of tunica interna designed to prevent backflow • Venous sinus has no muscle at all • coronary sinus or dural venous sinuses
Blood Distribution • 60% of blood volume at rest is in systemic veins and venules • function as blood reservoir • often called capacitance vessels • venous capacity = volume of blood the veins can accomodate • body at rest – much of the blood bypasses the closed capillary beds and enters the venous return circuit – this increases the blood volume in the veins • blood is diverted from it intimes of need • increased muscular activityproduces venoconstriction • hemorrhage causes venoconstriction to help maintain blood pressure • 15% of blood volume in arteries & arterioles
Veins & Venules • veins & venules have little tone and resistance • the arteriole communicates chemically with the venule to ensure that inflow and outflow surrounding the capillary region matches • much of the driving force on the blood (blood pressure) has been lost as it enters the veins • BP averages on 17 mm Hg in the veins • venous return is enhanced by many extrinsic factors • venous return = volume of blood entering the atria from the veins (pulmonary and systemic) 1. sympathetic activity – venous smooth muscle has an abundant nervous innervation by the sympathetic nervous division • can produce a small amount of constriction in the veins increasing venous BP and increasing the forces driving blood back to the heart • this contraction also decreases the amount of blood that can be held in the veins (decreases venous capacity) by decreasing the diameter of the vein itself • so less blood remains in the veins but is returned faster to the heart • skeletal muscle activity – contraction of skeletal muscles can push on the vein walls, decreasing their size and decreasing their capacity • venous valves – venous vasoconstriction and skeletal muscle contraction also drive blood away from the heart -evolved extensions off the endothelium – valves -these valves can shut off sections of veins to prevent back-flow towards the feet when standing • 4. respiratory activity– pressure in the chest is 5 mm Hg less than atmospheric • blood flowing through the thoracic cavity on the way back to the heart is exposed to subatmospheric conditions • this creates a pressure differential – drives more blood from the limbs = respiratory pump
Veins and gravity - gravity – when lying down, forces of gravity are equally applied to all veins -when standing, vessels below the heart become more subject to gravitational forces -so the veins increase their volume to counteract the increased volume -this reduces the amount of blood returning to the heart – decreases CO -also increases the pressure in the capillaries – forces more fluid out into the tissues from the blood -compensatory mechanisms – fall in MAP triggers the sympathetic NS to induce venous constriction to drive some of the pooled blood up toward the heart + skeletal muscle tone will increase to help propel blood to the heart
Varicose Veins • Twisted, dilated superficial veins • caused by leaky venous valves • congenital or mechanically stressed from prolonged standing or pregnancy • allow backflow and pooling of blood • extra pressure forces fluids into surrounding tissues • nearby tissue is inflamed and tender • Deeper veins not susceptible because of support of surrounding muscles