Mobility, what? Soft Tissue, who?
460 likes | 653 Vues
Mobility, what? Soft Tissue, who?. Brought to you by the LRMC. What is functional mobility? What is soft tissue and why do we care? What strategies can we implement in our daily lives to improve the quality of both? Q & A. Key Terms. Cervical Spine - Top portion of your spine

Mobility, what? Soft Tissue, who?
E N D
Presentation Transcript
Mobility, what?Soft Tissue, who? Brought to you by the LRMC
What is functional mobility? • What is soft tissue and why do we care? • What strategies can we implement in our daily lives to improve the quality of both? • Q & A
Key Terms • Cervical Spine • - Top portion of your spine • Thoracic Spine aka T-Spine • - Middle portion of your spine • Lumbar Spine • - Lower portion of spine • aka lower back • Neutral Spine • - Curves in all the right places • Scapular Region • - Upper cross of our back • Core/ Trunk • - That thing in the middle that holds you up
“Your eyes can only see what your brain knows” - Diagnosis & Treatment of Movement Impairment Syndromes
Everybody just breathe Seriously… just chill the eff out and… BREATHE!
Movements NOT Muscles • Ankle mobility (particularly sagittal) • Knee stability • Hip mobility (multi-planar) • Lumbar Spine stability • Thoracic-Spine mobility • Scapula stability • Gleno-humeral (shoulder) mobility • The first thing you should notice is the joints simply alternate between the need for mobility and stability as we move up the chain. • The ankle needs increased mobility, and the knee needs increased stability, etc.
The Process is Simple • Lose ankle mobility, get knee pain • Lose hip mobility, get low back pain • Lose thoracic mobility, get neck and shoulder pain, or low back pain • Looking at the body on a joint by joint basis just makes sense. • The ankle is a joint that should be mobile, and when it becomes immobile (lack of use through it’s full range of motion), the knee, a joint that should be stable, becomes unstable; the hip is a joint that should be mobile and it becomes immobile and this works it’s way up the body. The lumbar spine should be stable; it becomes mobile. • Joints have specific mobility and stability needs and when they’re not used very much or improperly, that immobility is more than likely going to cause a problem elsewhere in the body.
Compensations • When one joint sacrifices it’s stability for the mobility of another. This is known as a compensation. • Our bodies are magical creatures that will find a way to get the job done no matter what the cost. This is called dysfunction. • “Compensation Activation, • where in the body is your Limitation?” • - To the melody of School House Rock’s “Conjunction Junction”
Importance of Core strength/ Stability • “You can’t shoot a canon out of a canoe” • Whether you swim, run, or cycle, it is essential to have core stability to maximize performance and prevent injury. • The core of your body is where you derive your power; it provides the foundation for all arm and leg movements. Your core must be strong, flexible, and unimpeded in its movements to achieve maximum performance. • Motion is not an isolated event that occurs in one direction. Body movement is a complex event involving agonists and antagonists structures that work together to create motion and to stabilize the body in all three directional planes.
Why Machines Suck • “Machines make motor neuron morons” • Isolation exercises contribute to muscular imbalance. As a rule, the leg extension machine doesn’t work anything but the quadriceps. Unless you’re a bodybuilder going for ridiculous quads, you should avoid this machine at all costs. • Even if you supplement your “leg day” (arm, chest, back, and leg “days” are another pet peeve of mine) with some hamstring curls, calf raises, and glute pushes, you’re still contributing to muscle imbalance. • Each individual muscle might be strong in its own way, but they don’t work together.
Try to lift a heavy rock after a year of leg extensions, hamstring curls, and calf raises, and you won’t know how to coordinate each muscle to complete the movement. • Isolation exercises don’t improve your performance in functional activities (sports, hunting, lifting heavy things in real world terms); they increase your ability to only perform that specific isolation exercise. • A machine lover who can leg press a thousand pounds can’t squat the same amount, but a guy who squats a thousand pounds can probably double that amount on the leg press.
Yoga? Pilates? • Why should we have to choose? • Obviously some movement is better than no movement so if it was between yoga or nothing, I vote yoga. The same applies to Pilates • My biggest beef is the separation of the two and the often arbitrary prescription of one over the other as opposed to based on specific needs. • Flexibility, stability and strength in all the right places (functional mobility) should be the focus. Yoga and Pilates are just tools to get you to where you need to be. If one of the tools in the tool box hinders this goal than it is not the right tool for the job
Yoga • Yoga is based on the Eastern idea of moving energy through your body. The more freely the energy flows, the healthier and more energetic you feel. • Physical tension hinders the flow; over time, areas of tension in your body can become tight and rigid, even painful. • The goal of yoga is to keep the body supple through movement and stretching. • I love all that good stuff, however, often yoga is so focused on flexibility that a joint which should be stable i.e. lumbar spine, becomes flexible = NOT GOOD
Pilates • Pilates on the other hand is physical conditioning first and foremost • Pilates exercises stretch and strengthen and are unique in their ability to encourage coordination between the muscles that stabilize the body. • Once again, all good stuff but without the knowledge of potential compensations there’s an increased risk that certain muscle imbalances and compensations could be hammered in.
Importance of functional mobility • Everyone of any age or fitness level needs the ability to move their limbs and joints through their full range of motion as ordained by nature *Attainment of joint mobility, then, is regaining what was lost, not inventing something new.
Soft tissue • Would you rather be a stewing hen or a Thanksgiving centerpiece?? Srsly?
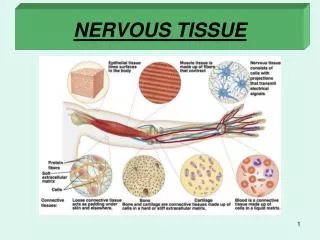
What is Soft Tissue? • The term soft tissue refers to tissues that connect, support, or surround other structures and organs of the body, not being bone. • Soft tissue includes tendons, ligaments, fascia, skin, fibrous tissues, fat, and synovial membranes (which are connective tissue), and muscles, nerves and blood vessels (which are not connective tissue). (Wikipedia) • In order to achieve optimal mobility we need to address areas of tightness in our soft tissue that could potentially restrict movement through our full range of motion
Soft Tissue Mobilization • The idea is to appeal to the autonomic nervous system in a way that leads to spontaneous release of the tight/ injured muscle, thus regaining the original resting length of that muscle. • It’s kind of a self-accupresssure technique. • Goal: permanent reorganization of scar tissue, the targeted muscle(s) return to the proper resting length, muscle imbalances are corrected, associated pain is decreased or eliminated altogether, and muscle performance is improved. • Basically, just keep in mind that all that soft stuff gets stuck and you need to work at unsticking it if you want to be awesome.
Foam rolling 101 • Cheaper than a Thai massage • Basic rules = If it hurts do it more…Do it til it doesn’t hurt • The End. • PS. It’s going to hurt…like a lot… but you feel all kinds of awesome later. The awesome is totally worth the pain • Foam rolling is like crack, Before you tried it, you never felt like you needed it but once you do, it’s over. You can’t live without it
That much sitting is just not natural Exercises to keep pain at bay for the desk jockey: Everyday mobility drills Neck Yaw (rotation) Neck surge (front to back) Wrist Pitch & Yaw Thoracic Surge (front to back) Pelvic Pitch (tilts front to back) 6. Pec stretch (do many times a day) 7. Shoulder blade squeeze
Where my runners be? • Do you, or have you in the past, experienced symptoms of? • Iliotibial Band Syndrome • Plantar Fasciitis • Patella Femoral Syndrome • Shin Splints • Hip pain STM (soft tissue mobilization) should be part of every runner’s maintenance program. Why? Simply put, repetitive stress takes its toll on the body. Rolling or releasing the tissue increases blood flow, eliminates trigger points, and facilitates optimal soft tissue mobility and range of motion.
In the diagram to the left, you can see common trigger points in the soleus. The X represents the trigger point & the red shaded area is the referred pain caused by the trigger point. • In the case of the soleus (sole of foot), restricted dorsiflexion (toes pointed up) could lead to other biomechanical compensations with running. • Initially, this often creates a dysfunctional and non-painful (DN) pattern. • Over time, this may eventually become a dysfunctional and painful (DP) pattern forcing runners to seek medical care.
Postural Deviations • Important: • While everyone will fall somewhere within this spectrum the most important thing to remember is always avoid: • Hyper-kyphosis (excessive curvature of the upper back) • AND • Hyper-lordosis (excessive curvature of the lumbar spine aka lower back, especially while standing! • Both of these can be dramatically improved by improving scapular and core stability
Okay, my brain hurts, now what? • Doing anything more than your currently doing will help you improve • Don’t stress about it. Feeling stressed about feeling good just doesn’t make a whole lot of sense
mobility drills for everyone! • FACT: For every mobility drill you do correctly you increase your awesomeness EXPONENTIALLY Scapular wall slide Supine bridge Reach, roll and lift Squat to stand Wall ankle mobilization Pull-back butt kick Cradle walk Overhead lunge walk Seated 90/90 stretch Bird Dog 11. Levator/ Scapulae upper trap stretch 12. High-knee walk 13. Reverse lunge w post-lateral reach 14. Quadraped/ seated thoracic rotation 15. Kneeling heel to butt stretch 16. Kneeling rock back 17. Behind back hand reach 18. Cat/camel Fire Hydrants Forearm/ wrist flexor stretch
Feeling better requires diligence • “The definition of insanity is doing the same thing over and over again and expecting different results." Einstein • Think about how many hours you spend sitting a week • Think about how many hours you spend standing with potentially bad posture a week • Think about how many hours you spend exercising a week (significantly less than the former two – can hardly contend in terms of rectifying postural weaknesses, asymmetries etc.) • Corrective exercise and taking care of our soft tissue will allow us to do the right thing more often so eventually it becomes the only thing we do. • This is when we start to feel and move better without even having to try… • Boooya!
When in doubt, soft tissue • So what do I do?? • *Soft Tissue Mobilization* • Static stretching • Foam roll • Dynamic stretching • Mobility drills *I know it’s a lot to remember but I think you can do it. I believe in you!!
What and how to foam roll • To get started What you need to get: 1) 6" foam roller (either the 1' long or 3' long version) 2) Marvin Gaye's "Sexual Healing" CD 3) A leopard-skin thong 4) Two quarts of baby oil to lube yourself up . Now what? If you don’t have the last 3 just yet, no worries. We can start with 1. Basically, you just use your body weight to sandwich the roller between the soft tissue to be released and the floor. Roll at a slow pace and actually stop and bear down on the most tender spots ("hot spots"). Once the pain in these spots diminishes, roll the other areas. In order to increase the pressure on the soft tissue, simply apply more of your body weight to the roller. The simplest way to do this is by either moving from working both legs at once to one leg, or by "stacking" one of your legs on top of the other to increase the tension.
Hamstrings: You'll want to try these with the feet turned in, out, and pointing straight ahead to completely work the entire hamstring complex. Balance on your hands with your hamstrings resting on the roller, then roll from the base of the glutes to the knee. To increase loading, you can stack one leg on top of the other.
Hip Flexors: Balance on your forearms with the top of one thigh on the roller. Roll from the upper thigh into the hip. Try this with the femur both internally and externally rotated. To do so, just shift the position of the contralateral pelvis. (In the photo, Mike would want to lift his right hip to externally rotate the left femur).
Tensor Fascia Latae and Iliotibial Band: Without a doubt, this one will be the most painful for most of you. In the starting position, you'll be lying on your side with the roller positioned just below your pelvis. From here, you'll want to roll all the way down the lateral aspect of your thigh until you reach the knee. Stack the opposite leg on top to increase loading.
Adductors: Balance on your forearms with the top of one of your inner thighs resting on the roller. From this position, roll all the way down to the adductor tubercle (just above your knee on the inside of your leg) to get the distal attachments.
Gluteus Maximus: Set up like you're going to roll your hamstrings, but sit on the roller instead. Roll your rump. Enough said.
Calves: This, too, is similar in positioning to the hamstrings roll; you're just rolling knee to ankle. Try this with the toes up (dorsiflexion) and down (plantarflexion). Stack one leg on top of the other to increase loading.
TibialisAnterior: This is just like the quad roll, but you're working on your shins instead. Peroneals: This one is similar to the TFL/ITB roll; we're just working on the lower leg now. Roll along the lateral aspect of the lower leg from the knee to the ankle.
Thoracic Extensors, Middle and Lower Trapezius, Rhomboids: With your arms behind your head (not pulling on the neck), lie supine with roller positioned in the middle of your back; your glutes should be on the ground. Roll upward, reversing direction when you reach the level of the armpits. This is an excellent intervention for correcting kyphosis.
LatissimusDorsi and Teres Major: Lie on your side with the same side arm overhead. The roller should be positioned at the attachment of the lat on the scapula in the starting position. You'll want to roll toward the attachment on the humerus (roll toward the armpit).
Thoracolumbar Fascia: With your arms folded across your chest, lie supine with the roller positioned under your midback. Elevate the glutes and roll from the base of the scapulae to the top of the pelvis. You'll want to emphasize one side at a time with a slight lean to one side.
Pectoralis Major and Anterior Deltoid: Lie prone with the roller positioned at an angle slightly to one side of the sternum; the arm on this side should be abducted to about 135° (halfway between completely overhead and where it would be at the completion of a lateral raise). Roll toward the humeral head (toward the armpit).