Download
1 / 12
130 likes | 374 Vues
Female Reproductive Pathology. Embryo/Anatomy: - Paired Mullerian ( paramesonephric ) ducts form and fuse to make tubes, uterus, upper vagina (default) - Wollfian ( mesonephric ) ducts regress All have same mesothelial ( coelemic origin) field defect. Infections :

E N D
Embryo/Anatomy: - Paired Mullerian (paramesonephric) ducts form and fuse to make tubes, uterus, upper vagina (default) - Wollfian (mesonephric) ducts regress All have same mesothelial (coelemic origin) field defect Infections: Herpes (HSV2): active vesicles (painful), latent neonatal infections (eye, rash, GI, probably die) (spotaneous abortions) Do Csection Do Tzank smear: multinucleated cells with intra-nuclear, “ground glass” inclusions MolluscumContagiosum Vaginitis: Candida: Cottage Cheese, itchy (DM, ABX, prego, IC) Trichamonas: yellow frothy, strawberry cervix Gardnerella: green fishy, clue cells Umbilicated tan papule Intracellular inclusion Pelvic Inflammatory Disease:infection beyond uterine corpus - Usually N. gonorrhea/Chlamydia low ab pain, tender to cervical manipulation (adhesions) - Complications: tuboovarian abscess, tube scarring ectopic preg., GI obstruction Clue cell: squamous cell covered in coccobacilli
VULVA Bartholin Cyst (usually gonorrhea) Rx: marsupulization Non-neoplastic Epithelial Disorders • Lichen Planus(purple, polygonal, pruritic, patches) Reticular=Wickham’s striae • Lichen Sclerosis (LS&A) • Pruritic, painful intercourse, NOT precancerous but ass. With increased risk of SCC • Thinned epidermis, sclerotic stroma (homogenized • Lichen Simplex Chronicus (LSC) • Thickened epidermis from chronic scratching (no atypia) • Hyperplasia/keratosis, acanthosis • CondylomaAcuminata(HPV 6,11) • Koilocytes: raisinoid nuclei with surrounding cleared area • Frequently regresses VIN: Vulvar Intraepithelial Neoplasm • Risks: old, lots o warts, IC Invasive SCC of Vulva • Masses on background of leukoplakia (esp ulcerated) • 2 types (same for VIN 3) Verrucous Variant: no infiltration, pushing margin. Make sure you biopsy deep enough
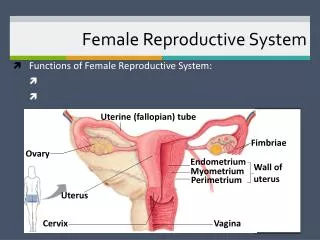
Vagina Vulva (cont.) Glandular Lesions of Vulva • Accessory Breast Tissue: along milkline, expands during pregnancy • Papillary Hidradenoma: benign from apocrine gland • Extramammary Paget: • pruritic, red, crusted, sharply demarcated. • No underlying Carcinoma • Histo: halo cells (PAS+, CEA+, EMA+, Mucin +) Malignant Melanoma: poorer prognosis b/c late presentation (S100, keratin +) Developmental Abnormalities - Congenital: imperforate hymen, double vagina - Gartner duct cyst: Wolffian derived remnant Vaginal Adenosis: mothers take DES glandular epithelium (velvety red) replaces squamous (pink) = adenosis clear cell carcinoma of vagina Vaginal Neoplasm: - 80% metastatic SCC from cervix • HPV 16 VaIN • Dx: cytology Prog: size and nodes EmbryonalRhabdomyosarcoma: <5yrs • Grape structure from vagina/ bleeding • Histo: see Z lines • High rate of surgical cure
Physiology: Squamocolumnar Junction SCJ at osEversion (Puberty) Transformation zone (post adolescent) Inversion (Menopause) transformation zone moves back up endocx canal Cervix Inflammations: Acute/Chronic Cervicitis: -Nonspecific: loss of acidosis (bleeding, sex, douching, ABX) - Specific: STDs Endocervical Polyps - common, benign, soft/mucoid - spotting or mass of cervical os (Rx: polypectomy) Nabothian Cysts: obstructed mucous gland Neoplasms: Low Grade (CIN I) High Grade ( CIN II-III) Cancer (10 years) Premalignant - CIN (cervical Intraepithelial Neoplasia) CIN I: 1/3 basal cells and atypia CIN III: full thickness (CIS) • Markers: Ki-67 (cell proliferation), p16 (unregulated cyclin E) see full thickness • - Culposcopy: acetowhite (dysplasia), mosaic (full thickness dysplasia) - Adenocarcinomain situ: hard to find (path same as CIN) Cancer - SCC: S&S: bleeding after coitus, advanced local invasion. Prog depends on TNM - die by invasion obstruct ureters renal failure - Rx: radical hysterectomy -Adenocarcinoma (more aggressive) Pap smear (Sensitive) + HPV DNA after 30 (Specific) = 99.5% sensitivity • HPV :Vaccine is 100% at 5 yrs (HPV 6/11/16/18) • Risks: young age at 1st intercourse, multiple partners, IC, BCPs, smoking • Infects immature, replicates mature (therefore, without transformation zone, need microtears to access immature cells) • HPV 6/11: episome (condylomas) • HPV 16/18: integrated into genome • E6: p53 E7: Rb
Proliferative Phase: Estrogen (simple tubules) Secretory Phase: Progesterone LH Surge: Ovulation Day 14 (subnuclear vacuoles) Late Secretory: everything in lumen Menstrual: stromal breakdown, hemorrhage Uterus Anovulatory Cycle: unopposed estrogen, no progesterone - irregular, dilated glands follicular cysts Inadequate Luteal Phase: abnormal corpus luteum = low progesterone corpus luteum cyst - Infertility with meno/amenorrhagia - Biopsy is >2 days behind clinical date Oral contraceptives: break through bleeding
Endometrial Polyps:sessile/pedunculated S&S: bleeding, benign Rx: surgery Endometrial Hyperplasia: Disordered proliferative pattern (us. Anovulatory) - Estrogen effect therefore diffuse EIN (Endometrial Intraepithelial Neoplasia): pre-neoplasia therefore focal (atypica) Lose PTEN Uterus (cont) Endometritis Acute (np): infections from delivery/miscarriage (GAS/staph) Rx: curette Chronic (PC): Chronic PID, IUD, Tb (3rd world), retained products of conception S&S: MMR, dysmeno, pain, infertility Endometriosis:endometrial tissue outside of uterus (us. Ovary) Adenomyosis: endometriosis in myometrium (watered silk) Adenomyoma: discrete mass of adenomyosis S&S: dysmeno, pain, infertility, scarring 2 theories: - metastatic: implant tissue - metaplasitc: same mullerian origin Tissue cycles with hormones bleeding toxic Cancer EndometrioidAdenocarcinoma (Type I) 45-55 yo fat women -unopposed estrogen (exogenous, endogenous, PCOD, infertility, DM, HTN) - S&S: DUB surgery - direct extension, late spread to nodes/ mets 2 pathways: PTEN mutation or microsatellite instability in KRAS (HNPCC/Lynch) Non-endometrioidAdenocarcinoma (Type II) old skinny sick women - EIC Grade 3 aggressive early spread through lymphatics - p53 Malignant mixed mullerian tumor (MMMT): - bulky polypoid mass Chocolate cyst and powder burn
Fallopian Tubes Uterus: myometrium Leiomyoma: Benign smooth mm Symptoms by location • Bleeding: submucosal - attenuation of endometrium • Pain/ sense of pelvic fullness: infarction, large mass • Urinary frequency: pressure against bladder • Infertility: may treat with myomectomy • Miscarriage: typically 2nd trimester Salpingitis: part of PID - Usually G/C - Pyosalpinx (pus), hydrosalpinx (fluid), tuboovarian abscess - Complications: adhesions, infertility, ectopic pregnancy Paratubal cysts:Mullerianremants at fimbriated end or in broad ligament -translucent, thin-walled Ectopic Pregnancy:Usually b/c of PID/adhesions, endometriosis DDx: torsion of ovary, appendicitis Measure hCG take out, if not may lead to fatal hemorrhage Adenocarcinoma:secondary tumor (esp serous ovarian) Leiomyosarcoma: 40-60yo Mass invading uterine wall OR polypoid mass in lumen Bad tumor (mitosis, atypic, necrosis) Metastasis by blood vessel invasion Endometrial biopsy: Aspirate : Pipelle tip Cut: curette tip Scrap: loop curette
Ovaries Benign Cysts: Follicular Cyst: - common, simple, no LH surge Corpus Luteum Cyst: - opening from released egg seals off, may hemorrhage/torsion Endometriosis: chocolate cyst Surface Epithelial Tumors (65-70%) 60yo women, asymp (general symp) until late (cachexia) Hereditary associations: BRCA1/2, Lynch (HNCC)- MSH2 Bilateral: serous>endometrial>mucinous No screening, CA-125 to trend, seeding of peritoneum Decreased risk by tubal ligation, BCP Serous Tumors Cystadenoma: benign, common, single layer Borderline: excrescences (seaweed), no invasion Adenocarcinoma: 65% bilateral, aggressive, poor prognosis - May present with ascites - Histo: psammoma, cribiform with central necrosis Mucinous Tumors Cystadenoma: least likely to be bilateral, most are benign Pseudomyxomaperitonei(us. Appendix): mucin in peritoneum= jelly belly Endometrioid Tumors Adenocarcinoma: may arise from endometriosis Same as endometriod Type I (PTEN, kras) can be synchronous If young: check for colon cancer (could be RAS/Lynch) Torsion of Ovary: (us. Cystic teratoma) S&S: sudden unilateral pain DDx: ectopic pregnancy Diagnose by US Polycystic Ovary Disease (PCOD; Stein-Leventhal Syndrome)commonest endocrine of repro age women - Oligomenorrhea(chronic anovulatory) -Virulization: hirsuite, muscley, bald, large clitoris - Polycystic ovaries: >12/ovary - obese, acanthosisnigricans, DM Rule out other endocrine
Ovaries (cont) Germ Cell Tumors Dysgerminoma (seminoma): Highly sensitive to radiotherapy 1/3 aggressive salpingooopherectomy fried egg appearance Endodermal sinus (yolk sac) AFP, Schiller-Duval (glomeruloid) Choriocarcinoma (gestat/non) b-HCG, aggressive, hemorrhagic Teratomas Dermoid (Benign Cystic Teratoma): repro age 2-3 cell lines. See hair/keratin/teeth Rokitanski nodule on cyst wall (all 3 layers) Immature Malignant Teratoma: girls/teens Immature tissue (fetal) Rapid growth and spread Monodermal (specialized) Teratomas: mainly 1 tissue Carcinoid: (primary= bilateral, mets = unilateral) serotonin flushing, diarrhea Struma ovarii: thyroid tissue weight loss, heart palpitations Sex Cord- Stromal Tumors Granulosa-Theca Cell Tumors - yellow, make estrogen - S&S: precocious puberty, endometrial hyperplasia and CA, proliferative breast disease - Diagnosis and monitoring: inhibin - Unpredictable Fibromas: common, white, hard, rubbery ball Associated with Meig’s: ascites, pleural effusion, ovarian fibroma Rx: resectfibroma Thecoma: makes estrogen, plump spindle cells with lipid droplet (stained red) Sertoli-Leydig Cell: makes androgens virulization Metastatic Carcinomas: Usually from other mullerian organs Extra-mullerian: breast, GI Krukenberk tumor:bilatmets of mucin, signet ring cancer cell, usually from GI
Causes of abortion: 1st tri: chromosomal 2nd tri: mechanical 3rd tri: fetoplacental unit Placenta Umbilical vein: carries oxygenated blood to fetus Umbilical arteries: carries deoxygenated blood away from fetus Amnion: baby side Chorion: maternal side (monochorion= identical twin) twin twin transfusion syndrome 3rd trimester villi: more dilated capillaries and looser stroma Placentation Problems Placenta previa: implantation over cervical os S&S: painless bleeding in 3rd trimester C section or death Abruptio placenta: premature separation of placenta c lot S&S: painful bleeding Complication of preeclapmsia More dangerous for the fetus Placenta accreta: attachment of placenta directly to myometrium therefore does not separate easily bleeding Asherman’s syndrome: no basalis from surgery, c sections, endometrial inflammation Placental infection/inflammation Chorioamnionitis, villitis, funisitis 2 routes of infection 1. Ascending from vagina/cervix (acute) GBS (agalactaie), 2. Hematogenous (transplacental) (chronic) Toxoplasmosis Other Rubella CMV HSV Hypertensive Disorders Preeclamsia: HTN, edema, protenuria HELLP: hemolysis, elevated liver, low platlets Eclampsia: pre + seizures
Invasive Hydatidiform Mole - Villi invades uterine wall and can embolize to distant organs (not mets) - If uterus ruptures life threatening - Chemo (if still want kids) or Hysterectomy Gestational Trophoblastic Disease Too much/too big • Uterus too big • Hyperemesis • HTN Higher in teens, 50s, Asians S&S: painless bleeding during 4th month Choriocarcinoma(us. African) - From complete mole (50%) abortion (25%) normal (22%) or ectopic pregnancy - bHCG (syncytiotrophoblasts) with no villous structures - Radiosensitive - Better behaved than non-gestational ones