Download
1 / 57
590 likes | 854 Vues
Department of General and Transplant Surgery Medical University of Lódź. SURGICAL TREATMENT OF FOCAL LIVER MASSES. P. HOGENDORF. HISTORICAL PERSPECTIVE. 1654 Francis Glisson – anatomy of th blood vessels of the liver

E N D
Department of General and Transplant Surgery Medical University of Lódź SURGICAL TREATMENT OF FOCAL LIVER MASSES P. HOGENDORF
HISTORICAL PERSPECTIVE • 1654 Francis Glisson – anatomy of th blood vessels of the liver • 1716 Berta – first described partial hepatectomy (stab wound, resection of portion of protruding liver) • 1908 J. Hogarth Pringle – Pringle's manoeuvre • 1957 – Couinaud - descriptions of the segmental nature of liver anatomy • 1950's operative mortality rate – 20 % ! • 1980's operative mortality rate – less than 5 %
PYOGENIC ABSCESS • Incidence 22/100.000 hospital admissions • 11 cases per million / year • male-to-female ratio is approximately 1.5 to 1
¾ involve right lobe of the liver ½ of hepatic abscesses are solitary 10% to 20% are sterile abscesses 40 % are polymicrobial Most common: E. coli & K. pneumoniae S. aureus, E. species, S. viridans, and Bacterioides species Potential routes of hepatic exposure to bacteria: Pathology and Microbiology: • biliary tree, • portal vein, • hepatic artery, • nearby focus of infection, • trauma
Presenting symptoms of hepatic abscess: • fever, • jaundice (25%), • right upper quadrant pain and tenderness (40-70%) • hepatomegaly all of the above presentation is present only 10%fever, chills, and abdominal pain are the most common • nonspecific symptoms (malaise, vomiting, diarrhea, cough, dyspnea, peritonitis secondary to rupture)
ALP is mildly elevated in 80% total bilirubin is elevated 20% to 50% Transaminases are mildly elevated about 60% • Leukocytosis 70% to 90% • Abnormalities of LFTs • Hypoalbuminemia • mild elevations of the prothrombin
The sensitivity of ultrasound in diagnosing hepatic abscess is 80% to 95%. • The sensitivity of CT in diagnosing hepatic abscess is 95% to 100%. • MRI does not appear to have any distinct advantage over CT in diagnosing hepatic abscess.
amebic abscess echinococcal cysts simple cyst Polycystic Liver Disease Differential Diagnosis • differentiating pyogenic abscess from other cystic infective diseases of the liver is important – differences in intreatment
broad-spectrum antibiotics covering gram-negative and gram-positive organisms and anaerobes: ampicillin + an aminoglycoside + metronidazole third-generation cephalosporin with metronidazole carbapenems TREATMENT • percutaneous catheter drainage has become the treatment of choice for most patients • percutaneous aspiration without the placement of a drain • liver resection mortality from 10% to 20%
E. histolytica other E. species - nonpathogenic Amebic Abscess • WHO estimated that 40 to 50 million people suffer from amebic colitis or amebic liver abscess worldwide • 40,000 to 100,000 deaths each year
the abdominal pain is typically constant, dull, and localized to the right upper quadrant. symptoms and tenderness may be epigastric or left sided if the abscess is located in the left pleuritic or shoulder pain can occur if there is irritation of the diaphragm. Clinical Features • 20 to 40 y old patient who has traveled to an endemic area • male-to-female ratio: > 10:1 • fever, chills, anorexia, • right upper quadrant pain, and tenderness and • hepatomegaly. • 1/3 patients have diarrhea despite an obligatory colonic infection. • jaundice is a rare presentation. • weight loss and myalgias
antiamebic antibodies that are present in 90% to 95% of patients. the EIA has a reported sensitivity of 99% and specificity greater than 90% in patients with hepatic abscess. Laboratory tests • moderate leukocytosis • anemia is common. • mild abnormalities of LFTs including albumin, prothrombin time, ALP, AST, and bilirubin levels are typical
CT is probably more sensitive than US, helpful in differentiating amebic from pyogenic abscess Nuclear medicine studies such as gallium scanning or technetium-99m liver scans Radiologic studies • US has a reported accuracy of approximately 90% when combined with a typical historyand clinical presentation
Treatment • Metronidazole (750 mg orally 3x per day for 10 days) curative in over 90% clinical improvement is usually seen within 3 days The mortality for all patients with amebic liver abscess is 2% to 4% When an abscess ruptures the mortality is reported to be from 6% to as high as 50%.
E. granulosus E. multilocularis and E. oligartus ¾ of hydatid cysts are located in the right liver ¾ are singular Hydatid Cyst • zoonosis that occurs primarily in sheep-grazing areas of the world • endemic in Mediterranean countries, the Middle East, the Far East, South America, Australia, New Zealand, and East Africa • the dog is a definitive host • no human-to-human transmission Echinococcus alveolaris
Dogs are the definitive host of E. granulosus, in which the adult tapeworm is attached to the villi of the ileum. • Eggs are passed (up to thousands of ova daily) and deposited with the dog’s feces. • Sheep are the usual intermediate host, but humans are an accidental intermediate host. Humans are an end stage to theparasite. In the human duodenum, the parasitic embryo releases an oncosphere containing hooklets that penetrate the mucosa, allowing access to the bloodstream. • Inthe blood, the oncosphere reaches the liver (most commonly) or lungs, where the parasite develops its larval stage known as the hydatid cyst
rupture of the cyst into the biliary tree or bronchial tree or free rupture into the peritoneal, pleural, or pericardial cavities can occur. Free ruptures can result in disseminated echinococcosis and/or a potentially fatal anaphylactic reaction. The most common presenting symptoms are: • abdominal pain, • dyspepsia, and vomiting. • hepatomegaly is the most frequent sign • jaundice - 8% • fever - 8%
but in elderly patients with small, asymptomatic, calcified cysts,conservative management is appropriate chemotherapy should generally be considered for widely disseminated disease or patients with poor surgical risk Treatment • primarily surgical • albendazole or mebendazole is effective in 20% to 30% of patients Recurrence rates after surgical treatment is less than 5 % in experienced centers
Focal Nodular Hyperplasia Other Benign Tumors NEOPLASMSSolid Benign Neoplasms • Liver cell adenoma (LCA) • Hemangioma
upper abdominal pain is common dramatic presentations with free intraperitoneal rupture and bleeding can occur quantifying the risk of rupture is difficult but it has been estimated to be as high as 30% to 50% and may be related to size malignant transformation into HCC Liver Cell Adenoma • predominantly found in young women aged 20-40 • relatively rare • chronic oral contraceptive use dramatically increases the incidence of this tumor • female-to-male ratio is approximately 11:1 • usually singular (multiple in 12% to 30%) • AFP level is normal
Liver Cell Adenoma • CT well-circumscribed heterogeneous mass. • MRI a well-demarcated mass containing fat or hemorrhage • primarily surgical treatment of symptomatic LCA (limited resections can be performed) acute hemorrhage need emergent operation
Liver Cell Adenoma Macroscopic aspect of liver adenoma with large intralesional hemorrhage Histology of hepatic adenoma arranged in plates that are two to three cells thick, separated by sinusoids
physical examination is usually unrevealing, and mild abnormalities of LFT may be found. AFP level is normal rupture, bleeding, and infarction are exceedingly rare No malignant transformations Focal nodular hyperplasia (FNH) • second most common benign tumor of the liver • FNH is usually a small (<5cm) nodular mass • central fibrous scar with radiating septa - 85 % • etiology is not known persistent symptomatic FNH or an enlarging mass should be considered for resection Contrast medium–enhanced CT MRI
Focal nodular hyperplasia (FNH) Contrast medium–enhanced CT: A delayed scan showed a non-enhancing scar with subtle enhancement of the capsule of the tumor MRI: on T2W image, mass appeared hypointense whereas the scar was hyperintense.
Focal nodular hyperplasia (FNH) Histology of a central stellate scar in FNH demonstrating thick-walled vessels (arrow) of a large arterial malformation surrounded by fibrous tissue Focal nodular hyperplasia with characteristic central fibrous region (arrow) and radiating fibrous cords
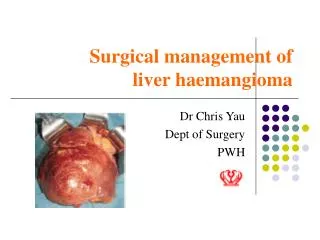
Hemangioma • the most common benign tumor of the liver • Female-to-male 3:1 • mean age of about 45 • usually singular • Usually less than 5 cm in diameter • occur equally in the right and left liver • > 5 cm are called arbitrarily “giant” hemangioma • Large compressive masses may cause vague upper abdominal symptoms. • Spontaneous rupture of liver hemangiomas is exceedingly rare. • An associated syndrome of • thrombocytopenia and consumptive coagulopathy known as Kasabach-Merritt syndrome is rare but well described • LFTs and tumor markers are normal
Hemangioma Cut section of two large hepatic hemangiomas showing central fibrosis and hyalin changes (arrows)
Hemangioma Radiological investigations: # Single-photon emission computed tomography (SPECT) # MRI # CT scan of the liver # Hepatic angiogram Post-contrast MR imaging of the liver demonstrating nodular peripheral enhancement of the right hepatic lobe lesion. First image demonstrates completely hypointense rounded lesion, which shows peripheral enhancement in the subsequent phases. This enhancement pattern is typical for liver venous malformations ("cavernous hemangiomas")
Other Benign Tumors • Nodular regenerative hyperplasia (NRH) • Mesenchymal hamartomas (Mhs) • Lipomas • Leiomyomas • Myxomas • Schwannomas • Lymphangiomas • Teratomas
risk factors: HBV infection, HCV infection, cirrhosis, smoking, alcohol abuse, age, chronic exposure to carcinogens such as aflatoxin, nitrites, hydrocarbons, solvents, pesticides, and vinyl chloride etc. inherited metabolic liver diseases such as hereditary hemochromatosis, a1 -antitrypsin deficiency, Wilson’s disease Primary Solid Malignant NeoplasmsHepatocellular Carcinoma • most common primary malignancy of the liver • over 1 million deaths annually worldwide • clearly related to the incidence of hepatitis B virus (HBV) infection • The highest incidence of disease (greater than 10 to 20 per 100,000) is found in Southeast Asia and tropical Africa • the lowest incidence (1–3 per 100,000) is found in Australia, North America, and Europe. macronodular cirrhosis
CLINICAL PRESENTATION • right upper quadrant abdominal pain, • weight loss, • a palpable mass • nonspecific symptoms: anorexia, nausea, lethargy • hepatic decompensation • Usually men 50-60 years of age • Rare presentations: - rupture with the sudden onset of abdominal pain followed by hypovolemic shock secondary to intraperitoneal bleeding - hepatic vein occlusion (Budd-Chiari syndrome) - obstructive jaundice, hemobilia, or fever of unknown origin - paraneoplastic syndrome, most commonly hypercalcemia, hypoglycemia, and erythrocytosis HCC largely metastasizes to the lung, bone, and peritoneum,
Cut section of a liver from a patient with Budd-Chiari syndrome demonstrating thrombus formation in a large hepatic vein (arrow)
DIAGNOSIS Radiologic investigation: • CT • MRI • US • Contrast medium–enhanced CT and MRI • Laboratory tests: • AFP level greater than 20 ng/mL in 75 % of HCC • Other: • percutaneous needle biopsies only in non-resectable cases
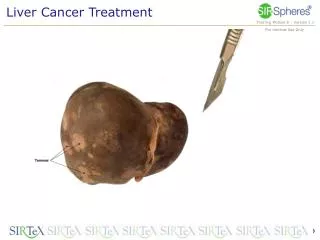
Hepatocellular Carcinoma Cut surface of a hepatocellular carcinoma without a capsule, infiltrating the liver parenchyma Cut section of a HCC with a mosaic pattern containing fat, solid nodules, necroses, fibrosis and cystic areas
Hepatocellular Carcinoma Histological aspect of a well-differentiated HCC showing bile production (arrows) Grade 1 HCC may be difficult to distinguish from liver-cell adenomas and atypical hyperplastic nodules
Liver resection is considered the treatment of choice for HCC Other successful treatments: - ablative techniques, - embolization techniques, - liver transplant Treatment • First step: to stage the tumor • Second step: assessment of liver function • Third step: treatment plan External beam radiation Chemotherapy Hormonal therapy Immunotherapy
Problems: lack of organ donors and need for chronic immunosuppression Treatment (2) • Patients with advanced cirrhosis (Child’s B and C) and early-stage HCC should be considered for transplant, whereas those • with Child’s A cirrhosis have similar results with transplant and resection and should probably undergo resection. Long-term survival rates in recent years have ranged from 25% to 75%.
risk factors: primary sclerosing cholangitis, choledochal cyst disease, recurrent pyogenic cholangitis. Cholangiocarcinoma • uncommon neoplasm • 1 to 2 per 100,000 in the United States • can develop anywhere along the biliary tree • 40-60 % involve the biliary confluence (Klatskin’s tumor) The clinical presentation of IHC is similar to that of HCC. If completely resected, 3-year survival rates range from 16% to 61% and 5-year survival rates range from 24% to 44%.
Other Primary Malignant Neoplasms • Hepatoblastoma • Sarcomas • Non-Hodgkin’s lymphoma • Malignant germ cell tumors • Primary hepatic lymphoma • neuroendocrine tumors • Epithelioid hemangioendothelioma Hodgkin’s disease
liver is a common site of metastases from gastrointestinal tumors Metastatic Tumors The most common malignant tumors of the liver are metastatic lesions: • colorectal cancer • tumors of the lung, • prostate, • breast, • pancreas, • stomach, • kidney, • cervix and ovary metastatic colorectal cancer isolated in the liver can be resected with the potential for long-term survival and cure
Diagnosis imaging studies (contrast-enhanced-CT, triphasic technique) LFTs CEA levels Colonoscopy – rule out local recurrence or metachronous lesions. Colorectal liver metastases • There are over 50,000 cases of colorectal liver metastases a year in the United States