Download
1 / 34
370 likes | 595 Vues
Abdomen. Anatomy of the Abdomen. Anatomy of the Abdomen (Abdominal Cavity). Four Quadrants. Midsternal line from the xiphoid process through the umbilicus to the pubic bone Horizontal line perpendicular to the first line through the umbilicus Quadrants named Right upper quadrant (RUQ)

E N D
Four Quadrants Midsternal line from the xiphoid process through the umbilicus to the pubic bone Horizontal line perpendicular to the first line through the umbilicus Quadrants named Right upper quadrant (RUQ) Right lower quadrant (RLQ) Left upper quadrant (LUQ) Left lower quadrant (LLQ)
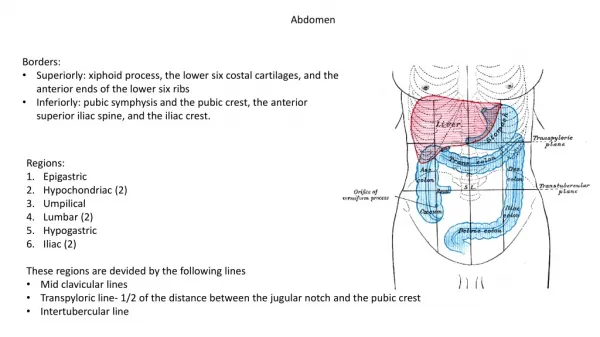
Nine Regions Extend the right and left midclavicular lines to the groin Horizontal line across the lowest edge of the costal margin Horizontal line at the level of the iliac crests
Anatomy of the Abdomen (cont.) Dividing the Abdomen into Four Quadrants Dividing the Abdomen into Nine Sections
History Taking of Problems of the Abdomen: GI Tract • How is the patient’s appetite? -Anorexia: lack of an appetite • Weight Loss • Any symptoms of the following? • Heartburn: a burning sensation in the epigastricarea radiating into the throat; often associated with regurgitation • Excessive gas or flatus
History Taking of Problems of the Abdomen: GI Tract (cont.) • Regurgitation: the reflux of food and stomach acid back into the mouth. • Vomiting; retching (spasmodic movement of the chest and diaphragm like vomiting, but no stomach contents are passed) • Ask about the amount of vomit • Ask about the type of vomit • Hematemesis: is blood or coffee ground emesis
History Taking of Problems of the Abdomen: GI Tract (cont.) • Ask patients to describe the abdominal pain in their own words • Ask patients to point with one finger to the area of pain • Ask about the severity of pain (scale of 1 to 10) • Ask what brings on the pain (timing) • Ask patients how often they have the pain (frequency) • Ask patients how long the pain lasts (duration) • Ask if the pain goes anywhere else (radiation) • Ask if anything aggravates the pain or relieves the pain • Ask about any symptoms associated with the pain
History Taking of Problems of the Abdomen: GI Tract (cont.) • Ask about prior medical problems related to the abdomen • Hepatitis, gallbladder problems, or pancreatitis, for example • Ask about prior surgeries of the abdomen • Ask about use of tobacco, alcohol, illegal drugs, as well as medication history • Ask about hereditary disorders affecting the abdomen in the history of the patient’s family
Medical problems related to the abdomen • Hepatitis: is a medical condition defined by the inflammation of the liver and characterized by the presence of inflammatory cells in the tissue of the organ. • Pancreatitis is the inflammation of the pancreas. Pancreatitis may be acute or chronic.
History Taking of Problems of the Abdomen: GI Tract (cont.) • Ask the patient about bowel movements • Frequency of the bowel movements • Consistency of the bowel movements (diarrhea vs. constipation) • Any pain with bowel movements • Ask about the color of the stools (white or gray stools can indicate liver or gallbladder disease) • Ask about difficulty
History Taking of Problems of the Abdomen: Urinary Tract • Ask about frequency (how often one urinates) and urgency (feeling like one needs to urinate but very little urine is passed) • Ask about any pain with urination • Ask about the color and smell of the urine; red urine usually means hematuria (blood in the urine) • Ask about difficulty starting to urinate
Physical Examination of the Abdomen: Inspection • Inspect the abdomen • Look at the skin: scars, striae (stretch marks), rashes, or lesions (Stretch marks or striae (singular stria), as they are called in dermatology, are a form of scarring on the skin with an off-color hue. They are caused by tearing of the dermis, and over time can diminish but not disappear completely)
Physical Examination of the Abdomen: Inspection • Look at the umbilicus: observe contour and location and any signs of an umbilical hernia (An umbilical hernia occurs when part of the intestine protrudes through an opening in the abdominal muscles. Umbilical hernias are most common in infants, but they can affect adults as well)
Physical Examination of the Abdomen: Inspection • Look at the contour of the abdomen: flat, rounded, protuberant, or scaphoid • Is the abdomen symmetric? • Inspect for signs of peristalsis (rhythmic movement of the intestine that can be seen in thin people) and pulsations (within blood vessels such as the aorta)
Physical Examination of the Abdomen: Auscultation • Auscultation is done before percussion and palpation since those maneuvers could potentially change the frequency and character of bowel tones. • Place the diaphragm over the abdomen to hear bowel sounds. These sounds are transmitted across the abdomen so it is not necessary to listen at multiple places. The normal frequency of sound is 5-34 sounds per minute.
Physical Examination of the Abdomen: Auscultation • Listen for bruits over the renal arteries, iliac arteries, and aorta by using the diaphragm of stethoscope
Physical Examination of the Abdomen: Percussion • Percuss over all four quadrants, listening for tympany (hollow sounds over the gastric bubble). Dullness is heard over the liver and spleen or a mass. • Percuss over the liver in both the right midclavicular line and at the right midsternal line • Midclavicular percussion should be 5–10 cm; longer than this indicates an enlarged liver • Midsternal line percussion should be 4–9 cm; shorter than this can indicate a small, hard liver
Physical Examination of the Abdomen: Light and Deep Palpation • Start palpating the abdomen using gentle probing with the hands; this reassures and relaxes the patient • Do not drag your hand over the surface of the skin • Identify any superficial organs or masses or tenderness • Use relaxation techniques to assess voluntary guarding • Tell the patient to breathe out deeply • Tell the patient to breathe through the mouth
Physical Examination of the Abdomen: Deep Palpation-Palpating the liver-(Standard technique) • Use your left hand to lift the lower rib cage and flank. • Press down just below the right costal margin with your right hand. • Ask the patient to take a deep breath. • You may feel the edge of the liver press against your fingers. A normal liver is not tender.
Physical Examination of the Abdomen: Deep Palpation-Palpating the liver-(hooking technique) • The “hooking technique” can be helpful when a patient is obese. • Place both hands, side by side, on the right abdomen below the border of liver dullness. • Press in with the fingers and go up toward the costal margin. Ask the patient to take a deep breath. The liver edge should be palpable under the finger pads of both hands.
Physical Examination of the Abdomen: Deep Palpation-Palpating the spleen • Use your left hand to lift the lower rib cage and flank. • Press down just below the left costal margin with your right hand. • Ask the patient to take a deep breath. • The spleen is not normally palpable on most individuals.
Special Tests-Shifting Dullness This is a test for peritoneal fluid (ascites). (Ascites: is a gastroenterological term for an accumulation of fluid in the peritoneal cavity) • Percuss the patient's abdomen to outline areas of dullness and tympany. • Position the patient on the right or left side. • Percuss and again outline areas of dullness and tympany. If the dullness has shifted to areas of prior tympany, the patient may have excess peritoneal fluid.
Special Tests-Rebound Tenderness- This is a test for peritoneal irritation and appendicitis. (Appendicitis a condition characterized by inflammation of the appendix) • Warn the patient what you are about to do (should be in supine position). • Press deeply on the lower right side of the abdomenwith your hand (at a 90-degree angle). • After a moment, quickly release pressure. • Ask if the client feels any pain. Normally, the client feels the pressure but no pain.
Special Tests-Rovsing's sign This is a test for appendicitis. • Applying hand pressure to the lower left side of the abdomen. • Pain felt on the lower right side of the abdomen upon the release of pressure on the left side indicates the presence of Rovsing's sign.
Special Tests-Psoas Sign This is a test for appendicitis. • Place your hand above the patient's right knee. • Ask the patient to flex the right hip against resistance. • Increased abdominal pain indicates a positive psoas sign.
Special Tests-Obturator Sign This is a test for appendicitis. • Raise the patient's right leg with the knee flexed. • Rotate the leg internally at the hip. • Increased abdominal pain indicates a positive obturator sign.
Special Tests-Costovertebral angle tenderness (CVA) (The costovertebral angle is the area on the lower back formed by the vertebral column and downward curve of the last posterior rib) CVA tenderness is often associated with renal disease. • Have the patient in sitting position. • Use the heel of your closed fist to strike the patient firmly over the costovertebral angles. • Compare the left and right sides.