Download
1 / 29
2.93k likes | 12.54k Vues
Basic principles of LAPAROSCOPIC SURGERY. Dr.Saifuddin Ahmed IMO Department of surgery, Unit 1 Chittagong Medical College Hospital. Contents. What is laparoscopy and its applications History Instruments ( details) Indications and contraindications Physiological changes

E N D
Basic principles of LAPAROSCOPIC SURGERY Dr.Saifuddin Ahmed IMO Department of surgery, Unit 1 Chittagong Medical College Hospital
Contents • What is laparoscopy and its applications • History • Instruments ( details) • Indications and contraindications • Physiological changes • Port of laparoscopy • Complications during operation • Commonly practiced laparoscopic surgeries • Some pictures of laparoscopic appendicectomy
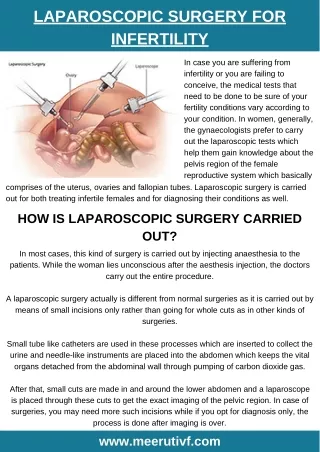
Definition • It is a minimally access procedure allowing endoscopic access to peritoneal cavity after insufflation of gas to create space between the anterior abd. Wall & viscera for safe manipulation of instruments & organs. TYPES • Intraperitoneal • Extraperitoneal • Abd wall retraction (gasless laproscopy) • Hand assisted (Hassans tech.)
HISTORY • George Kellingused cystoscope to observe abd organs of dogs— CYSTOSCOPY • 1910 – Swedish physician Hans Christian Jacobaeus used this procedure in man and coined the term – LAPAROSCOPY • 1987 – Mourett in France successfully removed a diseased gall bladder laparoscopically
INSTRUMENTS USED • Zero degree laparoscope • Cold light source (Halogen and Xenon lamp) • Camera ( 3chip camera commonly used with high resolution • Video monitor to display images • CO2 insuffulator • Long fine dissectors • Hooks and spatulas with cautery for dissections • Clip applicators • Needle holders • Veress needle • Trocars of different sizes – 10mm, 5mm • Suction irrigation apparatus • Reducers to negotiate smaller instruments through larger ports
Telescope • There are three important structural differences in telescope available 1. 6 to 18 rod lens system telescopes are available 2. 0 to 120 degree telescopes are available 3. 1.5 mm to 15 mm of telescopes are available
Trocar • The trocar has a blade with a shaft and body. • The body includes a pointed tip which makes the initial incision in the abdominal wall of the patient. (Trocar diameters range from 2mm-30 mm) Most common trocer is 5mm & 10mm
Optic Cables • These cables are made up of a bundle of optical fibers glass thread swaged at both ends. • The fiber size used is usually between 10 to 25 mm in diameter. • They have a very high quality of optical transmission, but are fragile.
Dissecting & Grasping Forceps • Atraumatic • KELLY atraumatic • Atraumatic, with hollow jaws • MANGESHIKAR Grasping Forceps, serrated
Laparoscopic Hook • It is used to separate adhesions, • Used for diathermy purpose, • To give traction to any organ.
Scissors • HOOK SCISSORS, single action jaws • METZENBAUM SCISSORS, curved, length of blades 12-17 mm, widely used as an instrument for mechanical dissection in laparoscopic surgery. • STRAIGHT SCISSOR can give controlled depth of cutting because it has only one moving jaw.
General instruments • Reusable three-piece design • Available in 2 mm, 3 mm, 3.5mm, 5 mm and 10 mm sizes, with lengths of 20 cm, 30 cm, 36 cm and 43 cm. • Choice of handle styles. • Fully rotating 360° sheath. • No hidden spaces that can trap operative blood and tissue debris.
Gas Insufflators • Gases used to create pneumoperitoneum: • Air • O2 • CO2 : most common • N2O : prefered for patients with cardiac disease • He, Ne, Ar ( new ) • Pneumoperitoneum is created upto 15mmHg which distends the abdominal cavity for proper visualization
Why CO2 is commonly usedto create pneumoperitonium ? • Readily available • Cheaper • Easily absorbed by tissues • Quickly released via respiration
Technique • Head end of the table is lowered to have easier insertion of needle scope • Pressure bandages are applied to both legs to improve the venous return • Ryle’s tube and foley’s catheter are essential before insertion of the trocars • Pneumoperitoneum is created using veress needle through umbilical incision
PHYSIOLOGICAL CHANGES co2 position Physiological changes pneumoperitoneum
Physiologic changes due to pneumoperitoneum • CO2 causes hypercarbia, acidosis and hypoxia • Pneumoperitoneum exerts pressure on the IVC, decreases the venous return and so the cardiac output • Increase the arterial pressure • Compromises the respiratory function by compressing over the diaphragm imparing the pulmonary compliance
Laparoscopic Port Positions • PRIMARY PORT POSITION • SECONDARY PORT POSITION • Attractive primary port is the umbilicus because of 1. central location and 2.the ability of the umbilicus to hide scars • Umbilicus is a naturally weak area due to absence of all the layers • Its location is at the midpoint of the abdomen’s greatest diameter. • Varying of operation • According to the surgeon preference
Basic Diamond Concept of Port Position • Mainly two port 5mm and 10mm port • Laparoscope is inserted through the umbilical port (10mm port) • Clip applicator 10mm port is essential • Additional ports ( 3-4) through trocars are placed depending on the procedures may be 5mm or 10mm port
Basic Diamond Concept of Port Position (5mm) • Port position for cholecystectomy (10mm) (5mm) • Port position for appendectomy
Commonly practiced laparoscopic surgeries • Laparocopic cholecystectomy • Laparoscopic appendicectomy • Laparoscopic inguinal hernia repair • Laparoscopic hysterectomy
Less commonly practiced laparoscopic surgeries • Laparoscopic perforation repair • Laparoscopic splenectomy • Laparoscopic vagotomy and gastrojejunostomy • Laparoscopic urologic surgeries
Diagnostic laparoscopyNeedle laparoscopy of 2mm sized becoming popular Indication • Acute pelvic conditions • Tubal pregnancy • Ovarian diseases • Infertility • Staging of the malignancy • Biopsy from the tumors • In chronic pain abdomen where ultrasound, endoscopies, barium studies are negative
CONTRAINDICATIONS 1. Absolute - none 2. Relative i) severe COAD ii) recent MI iii) ventriculoperitoneal shunts iv) Increased ICT v) extensive organomegalyvi) CHF
Advantages of laparoscopic surgery1. Less post operative pain2. Faster recovery time3. Shorter hospital stay4. Smaller scars5. Less internal scarring6. Less risk of wound infection and incisional hernia7. Better visualization of anatomy
Complications • Insertion Related : • Major vascular injury • GI Injury • Bladder injury • CO2 embolism • Abdominal wall haemorrhage • Post Insertional: • GI perforations • Laceration & bleeding from solid organs • Abdominal wall hernia • Pneumoperitoneal Related: • CO2 embolism • Hypercarbia • Respiratory acidosis • Subcutaneous emphysema • Renal failure • Venous thrombosis • Pneumothorax