Status Epilepticus
Status Epilepticus. Appendix 3 Debriefing Materials for Simulation Exercise. Status Epilepticus. Clinical or electrographic seizures lasting more than 30 min without full recovery of consciousness between seizures. Impending Status Epilepticus.

Status Epilepticus
E N D
Presentation Transcript
Status Epilepticus Appendix 3 Debriefing Materials for Simulation Exercise
Status Epilepticus • Clinical or electrographic seizures lasting more than 30 min without full recovery of consciousness between seizures
Impending Status Epilepticus • Continuous or intermittent seizures lasting more than 5 min without full recovery of consciousness between seizures • Treat as aggressively as confirmed status epilepticus
Subtle Status Epilepticus • Both the motor and EEG expression of seizures become less florid, however prognosis and therapeutic implications remain the same
Spectrum of Disease Impending Status Epilepticus Convulsive SE Subtle SE Nonconvulsive SE
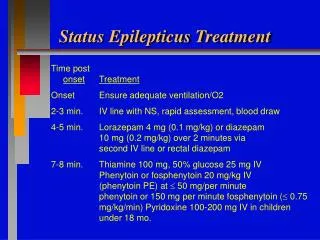
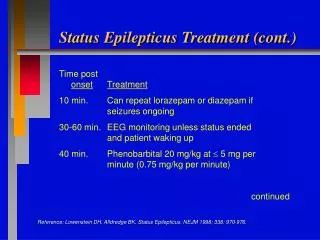
Benzodiazepines • Diazepam: enters CNS in 10 sec, lasts 20-30 min; rectal gel (10mg) effective in 75-90% of cases • Lorazepam: enters CNS in 2-3 mins; lasts 2-3 hours • Midazolam: 0.15 mg/kg load then drip @1-18 mic/kg/min iv, im, sl
Which Benzo Do I Use? • Lorazepam is preferred due to long activity • In the absence of intravenous access, diazepam can be given intramuscularly until access is established • Midazolam is generally reserved for refractory status epelipticus
Dilantin • Initiate intravenous load on presentation to ED for impending or established status epilepticus • Should I use phenytoin or fosphenytoin?
Dilantin • Phenytoin: • 20 mg/kg iv load @ 50 mg.min • onset in 20-30 mins but load is slow • low pH is damaging to soft tissue if IV infiltrates • Fosphenytoin: • 20 DPH equivalents iv or im • 8 mins for effect • Preferred for rapid load
Refractory Seizures • Barbiturates • Propofol drip • Midazolam drip • Valproic acid • Ketamine (only if CT head is negative for mass or hydocephalous) • ACEP Clinical Policies Committee and the Clinical Policies Subcommittee on Seizures. Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Seizures. Ann Emerg Med. 2004;43:605-625. • Chen, Wasterlain. Status epilepticus: pathophysiology and management in adults. Lancet Neurol 2006; 5: 246–56.
Consider Other Therapies • Eclampsia – Magnesium* • 6g loading dose over 15-20 minutes • 2g/h continuous infusion • INH overdose – pyridoxine • gram for gram dosing of pyridoxine • 5g iv when dose of INH unknown *Sibai. Diagnosis, prevention and management of eclampsia. Obstetrics & Gyn 2005;105(2):402-10.
Airway • Induction with • Etomidate may lower seizure threshold* • Propofol or barbiturates may be better • Paralysis is acceptable, but should obtain bedside EEG if long term paralysis initiated * Khalid, et al. J Electroconvulsive Therapy. 2006; 22:184-8.
Post Intubation Management • Consider higher ventilatory rates to compensate for lactic acidosis from convulsions • Paralysis may be helpful to reduce acidosis, but must be used with bedside EEG
Hemodynamic Support • Often necessary in refractory status epilepticus requiring barbiturates or propofol. • Intravenous fluids • Vasopressors as needed
Nausea Vomiting Dizziness Light sensitiviy Seizures Hyperpyrexia Hypotension Tachycardia Urinary retention Hemorrhage Ataxia Slurred speech Stupor Hepatitis Symptoms
Diagnosis • Clinical diagnosis • Should have an increased level of suspicion in refractory seizure • Bystander and EMS history very important
Laboratory • Anion gap acidosis • Elevated liver enzymes
Treatment • Support ABC’s • Activated charcoal • Treat seizures aggressively
Seizures • INH causes depletion of inhibitory neurotransmitter in brain (GABA) • Pyridoxine serves as cofactor to produce more GABA • Standard anticonvulsants are ineffective • Gram for gram dosing of pyridoxine • 5g iv when dose of INH unknown