Status Epilepticus
Status Epilepticus. Ives Hot, PharmD May 28, 2014 UW Medicine . Definition. Status Epilepticus (SE) 5 minutes of more of continuous clinical and/or electrographic seizure activity -OR- Recurrent seizure activity without recovery between seizures . Epidemiology .

Status Epilepticus
E N D
Presentation Transcript
Status Epilepticus Ives Hot, PharmD May 28, 2014 UW Medicine
Definition • Status Epilepticus (SE) • 5 minutes of more of continuous clinical and/or electrographic seizure activity -OR- • Recurrent seizure activity without recovery between seizures
Epidemiology • Estimated 100,000 to 200,000 episodes of SE in the United States annually • Mortality: 17-26% • Additional 10-23% of patients have disabling neurological deficits
Categorization • Convulsive • Associated with rhythmic jerking of extremities • Findings: tonic-clonic movements, mental status impairment, focal neurological deficits • Non-convulsive • Seen on electroencephalogram (EEG) without clinical findings • Refractory (RSE) • Patients who DO NOT respond to standard treatment • Received adequate doses of initial benzodiazepine • Second acceptable antiepileptic drug (AED)
Etiology • Acute: • Metabolic disturbances • Sepsis • CNS infection: meningitis, encephalitis, abscess • Stroke • Head trauma • Pharmacologic • Hypertensive encephalopathy • Autoimmune encephalitis
Etiology • Chronic: • Pre-existing epilepsy • Breakthrough seizure • Discontinuation/non-adherence to AED • Chronic ethanol abuse • CNS tumors • Remote CNS pathology ( stroke, abscess, TBI, cortical dysplasia)
Diagnostic Work-up • All Patients • Finger-stick glucose • Vital Signs • Head computed tomography • Lab: CBC, BMP, Ca, Mg, AED levels • Continuous EEG monitoring • Consider • Brain MRI • Lumbar puncture • Toxicology panel • Other lab tests
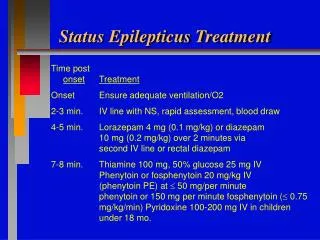
Treatment Goals • Emergently stop both clinical and electrographic seizure activity • Definitive control of SE should occur within 60 minutes
Treatment • Airway protection • Establish and support baseline vital signs • Establish medication route (Peripheral IV access), in order to: • Stop seizure • Establish euvolemia • Reverse thiamine deficiency/treat hypoglycemia • Other: labs, EEG, diagnostic testing, neurologic exam • Determine patient’s history
Drugs That Can Lower Seizure Threshold • Antibiotics • Imipenem, penicillins, cephalosporins, metronidazole, isoniazid • Antihistamines • Antipsychotics • Antidepressants • Bupropion • Tricyclics • Baclofen • Fentanyl • Ketamine • Lidocaine • Lithium • Meperidine • Propoxyphene • Theophylline
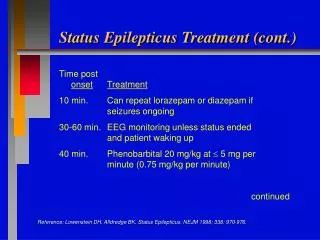
Emergent Initial Therapy • Agent of choice = Benzodiazepines • IV: lorazepam (Class I, Level A) • IM: midazolam (Class I, Level A) • PR: diazepam (Class IIa, Level A) • MOA: increase frequency of chloride channel opening in CNS GABA(A) receptors—decreasing neuronal excitability -VERSUS- • MOA of Phenobarbital: enhances GABA (A) chloride currents by increasing duration of chloride channel opening First-line medications control SE in 80% of patients when initiated within 30 minutes, but in only 40% if started after 2 hours of onset
Intranasal Midazolam • Administration • Use of atomizer • Use 5mg/mL injectable solution • Higher concentration injectable solution to minimize volume • Maximum dose is 1 mL per nare • Adverse effects • Burning/irritation
Urgent Control Therapy • Required following benzodiazepine administration in all patients who present with SE • UNLESS known cause of SE is identified and corrected • Goal 1: Rapid attainment of therapeutic levels of an AED and continued dosing for maintenance • Goal 2: To stop SE, if the patient failed emergent control
Fosphenytoin versus Phenytoin • MOA: stabilizes neuronal membranes and decreases seizure activity by increasing efflux or decreasing influx of Na ions across cell membranes in the motor cortex during generation of nerve impulses • Dosing difference • Fosphenytoin is converted to phenytoin on a 1:1 molar basis • Molecular weight fosphenytoin > Molecular weight of phenytoin • Greater weight of fosphenytoin must be given
References • Brophy GM, Bell R, Claassen J, et al. Guidelines for the evaluation and management of status epilepticus. Neurocrit Care. 2012;17(1):3-23. • Arif H, Hirsch LJ. Treatment of status epilepticus. Semin Neurology. 2008;28(3):342-354. • Stecker MM. Status epilepticus in adults. UpToDate Web site. http://www.uptodate.com/. Accessed May 23, 2014. • UpToDate Web site. http://www.uptodate.com/. Accessed May 24, 2014.