Download

1 / 63
700 likes | 1.08k Vues
VENTILATOR ASSOCIATED INJURIES,COMPLICATIONS AND INFECTIONS. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. Moderator:Dr.B.Kaur Speaker:Dr.Ashish. Ventilator-associated lung injury. Components BAROTRAUMA VOLUTRAUMA ATELECTOTRAUMA BIOTRAUMA OXYGEN TOXIC EFFECTS. Barotrauma.

E N D
VENTILATOR ASSOCIATED INJURIES,COMPLICATIONS AND INFECTIONS www.anaesthesia.co.inanaesthesia.co.in@gmail.com Moderator:Dr.B.Kaur Speaker:Dr.Ashish
Ventilator-associated lung injury Components • BAROTRAUMA • VOLUTRAUMA • ATELECTOTRAUMA • BIOTRAUMA • OXYGEN TOXIC EFFECTS
Barotrauma • Barotrauma - rupture of alveolus with subsequent entry of air into pleural space (pneumothorax) and/or tracking or air along the vascular bundle to mediastinum (pneumomediastinum). • Large tidal volumes and elevated peak inspiratory and plateau pressures are risk factors.
Barotrauma • Studies in patients with ARDS demonstrated that severity of underlying lung pathology is a better predictor of barotrauma than observed peak inspiratory pressure.
Barotrauma • The I:E ratio can be adjusted by increasing inspiratory flow rate, by decreasing tidal volume, and by decreasing ventilatory rate. • Attention to I:E ratio is important to prevent barotrauma in patients with obstructive airway disease (eg, asthma, chronic obstructive pulmonary disease).
Volutrauma • Volutrauma - local overdistention of normal alveoli. • Volutrauma has gained recognition over last 2 decades d/t importance of lung protection ventilation with low tidal volumes of 6–8 mL/kg.
Volutrauma • When a mechanical ventilation breath is forced into patient - positive pressure tends to follow path of least resistance to normal or relatively normal alveoli, potentially causing overdistention. • This overdistention l/t inflammatory cascade that augments or perpetuates the initial lung injury, causing additional damage to previously unaffected alveoli.
Volutrauma • The increased local inflammation lowers the patient's potential to recover from ARDS. • The inflammatory cascade occurs locally and may augment the systemic inflammatory response as well.
Volutrauma • Another aspect of volutrauma associated with positive ventilation is the shear force associated with the opening and closing effects on collapsible alveoli. • This has also been linked to worsening the local inflammatory cascade.
Volutrauma • PEEP prevents alveoli from totally collapsing at the end of exhalation and may be beneficial in preventing this type of injury.
ATLECTOTRAUMA • Lung injury a/w repeated recruitment and collapse • Preventable by using level of PEEP greater then lower inflection point of pressure-volume curve. • Also k/a low volume or low end expiratory volume injury
BIOTRAUMA • Pulmonary and systemic inflammation caused by release of mediators from lungs subjected to injurious mechanical ventiltion. • Mechanism – MECHANOTRANSDUCTION-physical forces are detected by cells and converted into biochemical signals • Injurious ventilatory strategy are as/w release of proinflammatory mediators like thromboxane B2, platelet activating factor and several cytokines.
Oxygen toxicity • Oxygen toxicity is a function of increased FIO2 and its duration of use. • Oxygen toxicity is due to production of oxygen free radicals, such as superoxide anion, hydroxyl radical, and hydrogen peroxide.
Oxygen toxicity • Oxygen toxicity can cause a variety of complications ranging from mild tracheobronchitis, absorptive atelectasis, and hypercarbia to diffuse alveolar damage .
Oxygen toxicity • No consensus has been established for the level of FIO2 required to cause oxygen toxicity • Use the lowest FIO2 that accomplishes the needed oxygenation.
Oxygen toxicity • It is adviced to attain an FIO2 of 60% or less within the first 24 hours of mechanical ventilation. • If necessary, PEEP should be considered a means to improve oxygenation while a safe FIO2 is maintained.
Lung Protective Strategy • ARDSNet Study - GOALS PaO2 55-80 mmhg T.V– 6 ml/Kg IBW RR up to 35 to maintain a pH > 7.30, if <7.15 then HCO3 Plateau Pressure < 30 cm H2O
How to set PEEP • Use PEEP FIO2 table from ARDSnet study • FiO2 .3 .4 .4 .5 .5 .6 .7 .7 .7 .8 .9 .9 .9 1.0 • PEEP 5 5 8 8 10 10 10 12 14 14 14 16 18 18-24 • This table is designed to be appropriate for the average patient, but sometimes PEEP needs to be individualized
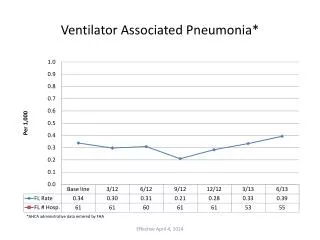
Ventilator associated pneumonia • Ventilator-associated pneumonia (VAP) is pneumonia that develops 48 hours or longer after mechanicalventilation is given by means of an Endotracheal tube or Tracheostomy.
Ventilator associated pneumonia • Ventilator-associated pneumonia remain important causes of morbidity and mortality despite • advances in antibiotics therapy, • better supportive care modalities, • and use of a wide-range of preventive measures
Ventilator associated pneumonia • The exact incidence of VAP is 6 to 20 fold greater than in Non-Ventilated patients. • VAP is associated with a higher crude mortality than other hospital-acquired infections (Level II).
How does the lung get infected ? • Sources of pathogens for VAP include • The environment (air, water, equipment,), and • Transfer of microorganisms between the patient and staff or other patients (Level II) • A number of host- and treatment-related factors, • Severity of the patient’s underlying disease, • Prior surgery, • Exposure to antibiotics • Exposure to invasive respiratory devices and equipment. (Level II).
How does the lung get infected ? • Aspiration of • oropharyngeal pathogens, or • leakage of secretions around the endotracheal tube are the primary routes of bacterial entry into the lower respiratory tract (Level II)
How does the lung get infected ? • Hematogenousspread from infected intravenous Catheters. • Bacterial translocation from the gastrointestinal tract lumen are uncommon pathogenic mechanisms (Level II)
How does the lung get infected ? • Infectedbio-film in the endotracheal tube, with subsequent embolization to distal airways, may be important in the pathogenesis of VAP (Level III) • The sinuses may be potential reservoirs of nosocomial pathogens but their contribution is controversial, (Level II)
Early: < 3 days of mechanical ventilation Typically community acquired agents Strep. Pneumoniae Other Streptococci MSSA Late: > 3 days from initiation of ventilation Gram negatives Pseudomonas Acinetobacter Klebsiella MRSA Early & Late VAP
Early vs late VAP • Time of onset of pneumonia is an important variable for the outcomes in patients with VAP . • Early-onset VAP, usually carry a better prognosis, and are more likely to be caused by antibiotic-sensitive bacteria. • Late-onset VAP are likely to be caused by multi-drug resistant (MDR) pathogens, and are associated with increased patient mortality and morbidity.
Clinical presentation of VAP • Usually suspected when a patient on mechanical ventilation develops • new pulmonary infiltrates • fever, • leucocytosis • purulent secretions. • Additional indicators maybe • increased Respiratory Rate, • increased minute ventilation, • decreased oxygenation, • or need of higher ventilatory support.
Diagnosis of VAP • Diagnosis is DIFFICULT because the clinical signs and x-ray features are non specific. • ONLY 50% OF PATIENTS WITH ALL ABOVE FINDINGS WILL HAVE VAP.
CLINICAL PULMONARY INFECTION SCORE: (CPIS) • Points are given for 7 variables • Temperature • WBC Count • PaO2/FiO2 • Chest X-ray • Quality of tracheal secretions • Progression of infiltrate • Culture of aspirate • Score >6 is considered suggestive of VAP. • BUT, recent studies have consistently shown low specificity and sensitivity of CPIS.
How Do We Diagnose? 2-1-2 • Radiographic evidence x 2 consecutive days • New, progressive or persistent infiltrate • Consolidation, opacity, or cavitation • At least 1 of the following: • Fever (> 38 degrees C) with no other recognized cause • Leukopenia (< 4,000 WBC/mm3) or leukocytosis (> 12,000 WBC/mm3) • At least 2 of the following: • New onset of purulent sputum or change in character of secretions • New onset or worsening cough, dyspnea, or tachypnea • Rales or bronchial breath sounds • Worsening gas exchange (↓ sats, P:F ratio < 240, ↑ O2 req.)
MICROBIOLOGY OF LOWER RESPIRATORY TRACT 2 TYPES OF METHODS: A] BRONCHOSCOPIC METHODS • i) BAL (broncho-alveolar lavage) • ii) PSB (protected specimen brush) B] NON BRONCHOSCOPIC (blind) METHODS • i) TRACHEO-BRONCHIAL ASPIRATION • ii) mini- BAL
BRONCHOSCOPIC METHODS • BAL(Bronchoalveolar lavage) • Involves infusion & aspiration of saline through a flexible fiberoptic bronchoscope that is wedged in a bronchial segment. • use atleast 140 ml saline to maximize yield • > 10 4 CFU/ml are taken as positive. • PSB( Protected specimen brush) • Minimises contamination during bronchoscopy, because the brush is contained in a protective sheath. • > 10 3 CFU/ml are taken as positive.
BAL vs PSB • PSB is 90% sensitive and 95% specific. • BAL is 80% sensitive and 85% specific.
NON-BRONCHOSCOPIC METHODS • TRACHEOBRONCHIAL ASPIRATION • blind method • basically it is the suction of ET secretions • > 10 5 CFU/ml are taken as positive. • Mini BAL • blind method • catheter is advanced till resistance is met, then saline is instilled, followed by aspiration of sample.
BRONCHOSPIC vs BLIND TECHNIQUES • Evidence suggests that Bronchoscopic sampling and culture methods tend to have higherspecificity, but the overall diagnostic accuracy is comparable. • Bronchoscopic methods have failed to show improvement in • mortality, • length of hospital stay, and • duration of mechanical ventilation when compared to blind methods. • It may, however, lead to a narrower antibiotic regimen.
The present CONSENSUS is:- • PROVIDED EMPIRICAL ANTIBIOTICS ARE STARTED AT THE TIME OF SUSPICION OF VAP, • EITHER OF THE TWO METHODS CAN BE USED FOR THE DIAGNOSIS.
Controversy : Use of Selective decontamination of digestive tract • SDD = use of prophylactic iv and oral antibiotics to sterilize the gut • In low resistance settings, efficacy of SDD is convincing. • In conditions of high antibiotic resistance (like in most Indian ICUs), SDD cant be recommended for prevention of VAP.
Modifiable Risk Factors • General prophylaxis. • Effective infectioncontrol measures: • staff education, • compliance with hand disinfection, • and isolation to reduce cross-infection with MDR pathogens should be used routinely (Level I)
Modifiable Risk Factors • Surveillance of ICU infections, • to identify and quantify endemic and new MDR pathogens, and preparation of • timely data for infection control and • to guide appropriate, antimicrobial therapy in patients with VAP, are recommended (Level II)
Intubation and mechanical ventilation. • Intubation and reintubation should be avoided, if possible as it increases the risk of VAP (Level I) • Noninvasive ventilation should be used whenever possible in selected patients with respiratory failure (Level I). • Continuous aspiration of subglottic secretions can reduce the risk of early-onset VAP, and should be used, if available (Level I)
Intubation and mechanical ventilation. • Heat–moisture exchangers decrease ventilator circuit colonization, but do not reduce the incidence of VAP.(Level I) • Orotracheal intubation and orogastric tubes are preferred over nasotracheal intubation and nasogastric tubes to prevent nosocomial sinusitis and to reduce the risk of VAP, (Level II)
Intubation and mechanical ventilation. • The endotracheal tube cuffpressure should be maintained at greater than 20 cm H2O to prevent leakage of bacterial pathogens around the cuff into the lower respiratory tract (Level II) • Contaminated condensate should be carefully emptied from ventilator circuits and condensate should be prevented from entering the endotracheal tube(Level II)
Intubation and Mechanical Ventilation. • Reduced duration of intubation and mechanical ventilation may prevent VAP and can be achieved by protocols to improve the use of sedation and to accelerate weaning (Level II) • Maintaining adequate staffinglevels in the ICU can reduce length of stay, improve infection control practices, and reduce duration of mechanical ventilation (Level II)
Enteral feeding. • Enteral nutrition is preferred over parenteral nutrition to reduce the risk of complications related to central intravenous catheters and to prevent reflux villousatrophy of the intestinal mucosa that may increase the risk of bacterial translocation (Level I)
Body position • Patients should be kept in the semi-recumbent position 30–45°. (Level I)
HOB Elevation > 30 Degrees on all Mechanically Ventilated Patients Contraindications • Hypotension MAP <70 • Tachycardia >150 • CI <2.0 • Central line procedure • Posterior circulation strokes • Cervical spine instability use reverse trendelenburg • Some femoral lines ie: IABP no higher than 30 degrees use reverse trendelenburg • Increased ICP, No higher than 30 degrees avoid hip flexion • Proning
Modulation of colonization: Oral antiseptics and antibiotics. • In prior administration of systemic antibiotics there should be increased suspicion of infection with MDR pathogens (Level II) • Prophylactic administration of systemic antibiotics for 24 hours at the time of Intubation is not recommended. (Level I)
Modulation of colonization: Oral antiseptics and antibiotics. • Modulation of oro-pharyngeal colonization by the use of oral chlorhexidine. Its routine use is not recommended (Level I) • Use daily interruption or lightening of sedation to avoid constant heavy sedation (Level II)
Stress bleeding prophylaxis, transfusion, and hyperglycemia. • There is trend toward reduced VAP with sucralfate, but if stress bleeding prophylaxis is needed either H2 antagonists or sucralfate is acceptable (Level I) • Transfusion of red blood cell and other allogeneic blood products should follow a restricted transfusion trigger policy; (Level I) • Intensive insulin therapy is recommended to maintain serum glucose levels between 80 and 110 mg/dl in ICU patients to reduce nosocomial blood stream infections, duration of mechanical ventilation, ICU stay, morbidity, and mortality (Level I)