Download
1 / 47
470 likes | 494 Vues
Explore new recommendations for cystitis and pyelonephritis management, including UTI pathogenesis, diagnosis, bacterial etiology, and treatment options. Understand asymptomatic bacteriuria screening guidelines and the latest research findings.

E N D
UPDATE UTIs: Cystitis and PyelonephritisManagement and New Recommendations Thomas M File, Jr MD MSc MACP FIDSA FCCP Chair, Infectious Disease Division Summa Health System Akron, Ohio; Professor of Internal Medicine, Chair ID Section Northeast Ohio Medical University Rootstown, Ohio
URINARY TRACT INFECTIONS • 12% of Women; 3% of Men yearly • 7- 8 million MD visits • 1 million ED visits; 100k hospitalizations • Catheter-associated UTI comprise up to 40% of all nosocomial infections • 1 million extra hospital days and $450 million per year • UTI: 25% of all infections in non-institutionalized elderly Taur & Smith. Clin Infect Dis 2007;44:769-74. Saint et al. Clin Infect Dis 2008; 46: 243-50. Hooton TM et al. Clin Infect Dis. 2010; 50: 625-683. Gulpt K et al. Clin Infect Dis. 2011; 52: e103-120.
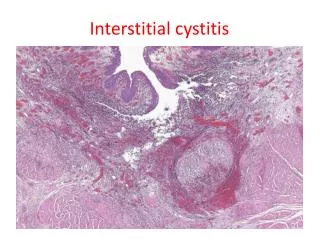
URINARY TRACT INFECTIONS: Pathogenesis • In women begins with colonization of the vaginal introitus by uropathogens from the fecal flora, followed by ascension via the urethra into the bladder. • Pyelonephritis develops when pathogens ascend to the kidneys via the ureters. • Pyelonephritis can also be caused by seeding of the kidneys from bacteremia. It is possible that some cases of pyelonephritis are associated with seeding of the kidneys from bacteria in the lymphatics.
UTI: Diagnosis • Urinalysis: • Clean catch mid stream • Pyuria-sensitive but not specific • Absence strongly against Cystitis • Bacteriuria • Nitrate test sensitive for detecting > 10(5) CFU of Enterobacteriaciae (lacks sensitivity for other organisms) • Culture • Standard: > 105 CFU • Differentiate from contamination • May be 102-104
Complicated vs Uncomplicated UTI • Uncomplicated: cystitis in nonpregnant women • Complicated: pyelonephritis or structural/functional abnormality that might reduce antimicrobial efficacy • Men • Children • Nosocomial infection Structural lesion, pregnancy, indwelling catheter or stent, neurologic bladder dysfunction, diabetes
UTI: BACTERIAL ETIOLOGY % Uncomplicated% Complicated Gram Negative E. coli70 - 9521 – 54 P. mirabilis1 – 2 1 – 10 Klebsiella spp. 1 – 2 2 – 17 Citrobacter spp. < 1 5 Enterobacter spp. < 1 2 – 10 P. aeruginosa < 1 2 – 19 Gram Positive Coagulase Neg staph5 – 101 – 4 Enterococci1 – 21 – 23 Group B strep < 11 - 4 Staph. aureus< 11 - 2 Nicolle LE. Drugs 1997;53:583-92.Czaja et al. Clin Infect Dis 2007;45:273.
What is appropriate therapy for a 55 year old asymptomatic diabetic female with >105E. coli in urine culture? a. Trimethoprim/Sulfamethoxazole (e.g. Septra, Bactrim) three DS tablets as a single dose b. Ciprofloxacin (Cipro) 250 mg po b.i.d. for 6 doses c. Nitrofurantoin (e.g. Macrobid) 100 mg po b.i.d. for three days d. None of the above; no therapy is required
ASYMPTOMATIC BACTERIURIA SCREENING AND TREATMENT NOT INDICATED Premenopausal, Nonpregnant or Diabetic Women1 Older persons whether living in Nursing Homes or in the community 2 Spinal cord Injury 2 Catheterized patients 2 1 ACOG Bulletin #91. Obstet Gynecol 2008;111:785 2Nicolle et al. IDSA Guidelines. Clin Infect Dis 2005;40:643-50.
ASYMPTOMATIC BACTERIURIA • DEFINITION Single Catheter Specimen with > 105 Bacteria Women: 2 CCU Specimens with same Bacteria (> 105 ) Men: Single CCU specimen with > 105 Bacteria • SCREENING AND TREATMENT INDICATED Urologic Surgery (Including TURP) Pregnancy (if untreated 33% go on to pyelonephritis) Nicolle et al. IDSA Guidelines. Clin Infect Dis 2005;40:643-50
Prevalence of Asymptomatic Bacteriuria Population Prevalence Healthy premenopausal women 1-5% Pregnant women 2-10% Postmenopausal women (50-70) 3-9% Diabetic women/men 9-27/4-19% Elderly (>70) in community: W/M 25-50/15-40% Spinal cord injuries 23-90% Indwelling catheters short term 9-23% Long term 100% Nicolle L et al. Clin Infect Dis 2005; 40: 643-54 (IDSA Guidelines for asymptomatic bacteriuria in adults)
ASYMPTOMATIC BACTERIURIA in Young Women • RCT of 673 young women (18-40) • No therapy vs antimicrobial (based on culture) • RESULT: • Recurrence: No therapy 13% vs Therapy 47% (p< 0.001) • CONCLUSION: No benefit to treat. AB should not be treated in young women and it may play a protective role in preventing symptomatic recurrence Cai T et al. Clin Infect Dis 2012; early access July 5
Reflexive Urine Culture based on UA • Less Ucx being performed. • CA-UTI rates decreased • No decrease total antibiotic days in hospitalized inpatients
ASYMPTOMATIC BACTERIURIA • SCREENING AND TREATMENT NOT INDICATED Premenopausal, Nonpregnant or Diabetic Women1 Older persons whether living in Nursing Homes or in the community 2 Spinal cord Injury 2 Catheterized patients 2 • SCREENING AND TREATMENT INDICATED Urologic Surgery (Including TURP) Pregnancy (if untreated 33% go on to pyelonephritis) 1 ACOG Bulletin #91. Obstet Gynecol 2008;111:785 2 Nicolle et al. IDSA Guidelines. Clin Infect Dis 2005;40:643-50.
Case: 22 y/o female presents with acute dysuria. Afebile; U/A: loaded with WBCs and bacteria. What is best option for Therapy? Amoxicillin for 10 days Ciprofloxacin for 10 days Ciprofloxacin for 3 days Trimethoprim-sulfamethoxazole for 10 days Trimethoprim-sulfamethoxazole for 3 days
Recent IDSA Guidelines • Cystitis-Empirical Therapy • Preferred Agents • Nitrofurantoin 100 mg bid X 5 d (avoid if pyelo) • TMP/SMX DS bid x 3 d • Fosfomyin 3 Gm X 1 (avoid if pyelo) • Pivmecillinam 400 mg bid X 5 d (avoid if pyelo) • Alternative • Fluoroquinolone o • Beta-lactams (avoid amoxicillin for empirical therapy; “amoxicillin-clavulanate appropriate choice”) www.idsociety .org; Clin Infect Dis. 2011; 52: e103-e120
Case: 32 y/o healthy woman with frequent UTIs. She is monogamous with a single male partner who always uses condoms. Which of the following would likely to decrease her frequency of UTI? • Urinate after intercourse • Have partner discontinue spermicide use with condoms • Drink a glass of cranberry juice daily • Stop wearing pantyhose
RISK FACTORS FOR UTIIN YOUNG WOMEN • 1 Month Frequency of Sexual Intercourse • OR 5.8 (3.1 - 10.6) • 1 Year Spermicide and Diaphragm Use • OR 1.8 (1.1 -2.9) • Age < 15 years at First UTI • OR 3.9 (1.9 -8.0) • History of UTI in Mother • OR 2.3 (1.5 - 3.7) • Genetic Factors • Nonsecretors of ABH blood-group antigens • Genetic Polymorphisms of Toll-like receptors (TLR) 4 and 11and Heat Shock ProteinsInherited reduced CXCR1 expression Scholes et al. J Infect Dis 2000;182:1177
RECURRENT CYSTITISIN YOUNG WOMEN • > 90% Are Due to Reinfection • Urologic evaluation Not Indicated unless Relapse Documented1 • Management Options: • Aggressive hydration counterproductive • Cranberry tablets have some efficacy short term vs. placebo 2,3 1 Albert et al. Cochrane Database of Systematic Reviews (3) CD001209, 2004. 2 Jepson et al. Cochrane Database of Systematic Reviews (2) CD001321, 2004. 3 McMurdo et al. J Antimicrob Chemother 2009; 63:389.
RECURRENT CYSTITIS IN YOUNG WOMEN: Management Options: • Avoid spermicides • Post coital voiding-variable results • Self-initiated Rx on Recurrence of Symptoms • Give women dipsticks from office or use home kits?1,2 • Antibiotic Prophylaxis Before Bedtime or Just After Sexual Intercourse (T/S, NTF)or Daily3 (85-95% Effective) • 6 – 12 months, then reassess • Recent study: daily NFT better than cranberry pills, estrogen therapy, and symptomatic self treatment (Eells et al. Clin Infect Dis 2014; 58: 147) • 1 ACOG Bulletin #91. Obstet Gynecol 2008;111:785.; 2 Johannes. Testing at Home for UTIs. Wall Street Journal 6/9/2009 3 Eells et al. Clin Infect Dis. 2014; 58: 147..
RECURRENT CYSTITISIN YOUNG WOMENManagement Options: • Three Question Evaluation: • 1. Do you think you have another UTI? • 2. Do you have burning with urination? • 3. Do you have vaginal Irritation? • If Yes, Yes, No: Treat for recurrent UTI Suzanne Geerlings, Netherlands. IDSA 2011
RECURRENT CYSTITISIN YOUNG WOMENPrevention Options: • Low dose ABX • Effective but assoc with emerging resistance • Cranberry juice/tablets • Variable efficacy but worth trying • Estrogen • If PAP shows atrophic vaginitis • Lactobacilli • Effective is small studies Suzanne Geerlings, Netherlands. IDSA 2011
Case: 55 y/o female with prolapse bladder and recurrent cystitis presents with 2 days of dysuria. Treated for 4 UTIs in past year. Afebile; U/A: loaded with WBCs and bacteria. Culture: E. coli resistant to SXT/TMP, Amox/clav, Nitrofurantion, Cefepime, Cipro; susceptible to imipenem. What is best option for Therapy? Linezolid po Fosfomycin po Carbenicillin po Doxycycline po
Case: UTI in outpatient E. coli = ESBL (Extended Spectrum Beta-lactamase) producer. Most are susceptible to fosfomycin Oral agent for cystitis. Effective for most E.coli including ESBL organisms Therapy: Uncomplicated cystitis: 3 gm as single dose Complicated UTI: 3 gm every 2-3 days for 3 doses Prostatitis: 3 gm every 2-3 days for 21 days
Fosfomycin (Monurol™) • Phosphonic acid derivative, approved in US for single dose Rx of UTI • Inhibits cell wall synthesis (cidal) by inactivating pyruvyltransferase, which is critical in the synthesis of cell walls by bacteria • Available as sachet containing 3 g fosfomycin to be dissolved in H2O • Bioavailability: 30% (fed) - 37% (fasting) • Excreted unchanged in urine and feces • Mean urine concentration 706 mcg/ml • T1/2 5.7 h • Pregnancy Category B • Not active against most P. aeruginosa
Etiology and sensitivity of uropathogens in uncomplicated UTI in women • Multicenter study, 803 woman • E. coli 80%; S saprophyticus 4.4%; P mirabilis 4.3%; enterococcus 3.2%; K pneumoniae 2.3% • Susceptibility E coli: • Fosfomycin 97%; nitrofurantoin 94%; cipro 88%; cotrimoxazole 66%; amox/clav 75%; ampicillin 45%; Pigrau et al. Med Clin Oct 2010
Case: 35 y/o female with dysuria, frequency, urgency, fever of 101 F, left-sided flank pain. Other vital sign. WBC 14,800. UA positive for leukocyte esterase and nitrites. Preg test-neg. Which is most appropriate choice? Ciprofloxacin po Fosfomycin po Nitrofurantion po Ceftriaxone IV
Recent IDSA GuidelinesAcute Uncomplicated PyelonephritisRecommended Antimicrobials - Outpatient Rx • Urine culture and antibiotic susceptibility in all • If prevalence of resistance of community uropathogens not known to be >10%: • Oral ciprofloxacin 500 mg twice daily for 7 days with/without initial 400 mg IV dose* (A-I) • Oral ciprofloxacin extended release 1000 mg once daily for 7 days OR levofloxacin 750 mg once daily for 5 days with/without initial IV dose* • If susceptible, TMP/SMX DS twice daily x 14 days with/without initial IV dose* • Oral ß-lactams are less effective (if used, give initial IV antibiotic*
Recent IDSA GuidelinesAcute Uncomplicated PyelonephritisRecommended Antimicrobials – Inpatient • Preferred Agents (depends on local resistance) • Oral Cipro 500 mg bid X 7d if not requires admission and local resistance <10% (alt: IV FQ or ceftiaxone or aminoglycoside X1); alter: cipro 1 gm or levo 750 Qd; TMP/SMX DS bid if susceptible • If FQ resistance > 10%: IV Ceph or aminoglycoside • IF requires hospitalization: Extended spectrum Beta-lactam (e.g. piperacillin/tazobactam, cefepime) +/- aminoglycoside Gupta K et al. Clin Infect Dis. 2011;52:e103-e120
UTI IN THE ELDERLY • Most often associated with catheters • Yearly Incidence in Noncatheterized patients: Men: 0.11 Women: 0.33 – 0.46 • Treatment of asymptomatic bacteriuria: • NO decrease in symptomatic UTI • NO decrease in incontinence • INCREASED adverse effects, resistance development and $$$ Nicolle. Curr Opin Infect Dis 2005;18:49-53. Dairiki, Shortliffe and McCue. Am J Med 2002; 113 (1A):1A-55S
Catheter-Associated UTI • 25% Hospitalized Patients Get Catheter • Incidence of Bacteriuria is 3 - 10% per Day • UTI Extends Hospital Stay: 1 - 3 Days • CMS won’t Pay! • DO NOT PLACE CATHETER • Saint et al. Clin Infect Dis 2008; 46:243. • Hooten et al. IDSA Guidelines for CA- UTI. Clin Infect Dis 2010; 50:625.
Preventing CA-UTIInstitutional Responsibilities: Monitor, Report and Reduce • Aseptic insertion and proper maintenance • Develop guidelines for early removal • Automatic stop orders; nurse-driven or electronic physician reminders • Silver-alloy coated catheters? Hooten et al. IDSA Guidelines for CA-UTI. Clin Infect Dis 2010; 50:625. Lo et al. SHEA/IDSA Strategies to Prevent CA-UTI in Acute Care Hospitals. Infect Cont Hosp Epidemiol 2008. 29: S41.
FOLEY CATHETERS:ALTERNATIVES • Diapers • Scheduled Voiding • Intermittent Catheterization1 • Sterile vs ‘Clean” techniques2 • Condom Catheters?3 • Suprapubic catheters? 1Bladder management in spinal cord injury. J Spinal Cord Inj 2006;29:527. 2Moore et al. Clin Rehabil 2006: 20:461. 3Saint et al. J Am Geriatrics Soc 2006;54: 1055-61. Hooten et al. IDSA Guidelines for CA-UTI. Clin Infect Dis 2010; 50:625.
Prophylaxis for CA-UTI • Systemic antimicrobials NO • Methenamine salts NO • Cranberry products NO • Daily meatal care NO • Catheter Irrigation NO • Routine catheter change NO • Screening and Rx for Asymptomatic bacteriuria NO Hooten et al. IDSA Guidelines for CA-UTI. Clin Infect Dis 2010; 50:625.
82 y/o female transferred from LTCF with chest pain; has acute MI. Has foley catheter. Afebrile; + pyuria; Culture: 105 Klebsiella pneumoniae Course of action? • Start antimicrobial • Await susceptibility test and chose most cost effective agent for therapy • No antimicrobial therapy warranted • Methenamine
UTI in LTCF • CULTURE SHOULD NOT BE PERFORMED FOR ASYMPTOMATIC RESIDENTS!!!!![A-I] • 10-50% or residents have >105 cfu/ml • Prospective studies have shown no benefit to treat • Pyuria or positive dipstick for leukocyte esterase not helpful unless negative • In non-cath pats, reserve U/A and culture for those with UTI symptoms [A-II] LTCF Long Term Care Facility. From Infect Dis Society Am Guidelines. Clin Infectious Dis. access via www.idsociety.org
Foley-associated UTI: • Treat only if symptomatic • Most predictive: change in character of urine, change in MS, fever • Base antimicrobial on susceptibility results; usually 10-14 days • Prevention • Works • Keep closed system • Silver Coated catheters (? benefit) • Of NO benefit • Periodic irrigation • Systemic antibiotics (possibly if short duration catheter) • Topical meatal antimicrobials
Which of the following is the best option for a 72 y/o female with chronic foley-catheter and suspected urosepsis? • Treat with ciprofloxacin, then change catheter • Obtain a urine culture and start broad spectrum antimicrobial, then change the catheter • Change the catheter, then obtain urine culture, start broad spectrum antimicrobial.
UTI in LTCF • If long term Cath, evaluate if suspected urosepsis (I.e., fever, chills, delirium) especially if recent catheter change [A-II] • If long term cath and suspected urosepsis, CHANGE CATHERTER PRIOR TO SPECIMEN COLLECTION AND INSTITUTION OF ANTIBIOTICS [A-II] • Prospective randomized trial demonstrated replacement of catheter prior to antimicrobial therapy was associated with imporved outcomes (Raz R, Schiller D, Nicolle LE. J Urol 2000 Oct;164(4):1254-8.) From Infect Dis Society Am Guidelines. Clin Infectious Dis. 2008; access via www.idsociety.org
82 y/o female transferred from LTCF with fever, decrease mental status; WBC-15,000. Exam unremarkable. Has long-term foley catheter: + pyuria; Treated initially with ciprofloxacin. Day #3 lab reports culture with > 100,000 E. coli resistant to ciprofloxacin but susceptible to all other agents tested. What is the appropriate choice now? Stop ciprofloxacin and start: • Cefepime • Ampicillin • Piperacillin/tazobactam • Imipenem
De-escalation Susceptibility results used to more specifically target microbiological results; narrowing the antibiotic spectrum by changing from a broad spectrum agent to a narrow spectrum agent or by eliminating a drug from combination therapy. Should ideally occur as soon as possible, but within 48 hours of the availability of culture results. Benefits include reduced bacterial resistance, decreased incidence of bacterial, viral, and fungal superinfections, limited exposure to unnecessary drug therapy and the associated risks decreased costs.
TREATMENT OF CA-UTI • Obtain pre-treatment urine culture after removing old catheter • Broad spectrum initial therapy • Account for recent antibiotic therapy, local sensitivity patterns • Narrowest spectrum agent to which pathogen(s) are susceptible • 7 days therapy for rapid responders • 14 days therapy for slow responders Hooten et al. IDSA Guidelines for CA-UTI. Clin Infect Dis 2010; 50:625.
UTI: Novel Approaches • ? Helpful over short term • Cranberry products1 • lactobacillus products (topical and oral) • Oral “not noninferior” in post menopausal women (Beereppot et al. Arch Intern Med 2012; 172:704-12) • Vaccine trials2,3 • SolcoUrovac (mixed GNRs; whole cell) • Uro-Vaxom (18 serotypes E. coli) • FimH, FimC (Type 1 Fimbriae from E. coli) • Pap D, Pap G (P fimbriae fromE. coli) • Uropathogenic E coli • Colonization with “benign”E. coli3 1 Schaeffer et al. J Urol 2005,173-111-2.; 2 Stapleton, J Urol 2004; 171: 1686-7.; 3. Brumbaugh AR Expert Rev Vaccines 2012; 11: 663-76; 4. Darouiche et al. Clin Infect Dis. 2005; 41: 1531-4.
Findings of Cranberry Juice • Cranberry juice fails to prevent recurrent UTI in college women • Clin Infect Dis 2011; 52:23-30. • Cranberry juice prevented recurrent UTI • Clin Infect Dis. 2011: 52: 1393-4 • Cranberry juice: non significant reduction in UTI in premenopausal women • But trend in reduction of P-fimbriated E. coli (0.07) • Mayo Clin Proc 2012; 87: 143-50. • Cranberry Juice: effective • Cochrane systematic review 2008
CRANBERRY JUICE/TABLETS • Laboratory studies have demonstrated that cranberry juice inhibits adherence of uropathogens to uroepithelial cells. • The mediators of this anti-adherence effect may be fructose, which could interfere with adhesion of type 1 fimbriated E. coli to uroepithelium and proanthocyanidins, which can inhibit adherence of P-fimbriated E. coli. • Therapeutic dose requires ‘a lot’ of juice; consider tablets Zafriri D. et al. Antimicrob Agents Chemother 1989; 33:92.
UTI: Take Home Messages • Don’t treat asymptomatic bacteriuria • Unless Pregnancy; Urologic Surgery • Uncomplicated cystitis • Fluoroquinolone NOT Drug of choice • Consider: TMP/SXT; Nitrofurantoin; Fosfomycin • Recurrent UTI • Consider strategy of ‘preventative’ therapy • Foley Cath associated • Don’t treat asymptomatic • Remove ASAP • Don’t plan scheduled replacement if chronic; don’t manipulate if not necessary