Download
1 / 19
270 likes | 779 Vues
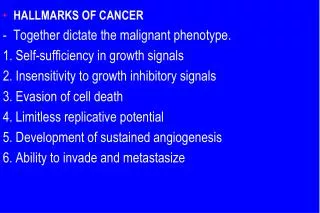
Hallmarks of Cancer. Ellie Seaby. What is cancer?. “All cancers arise as a result of changes that have occurred in the DNA sequence of the genomes of cancer cells” Stratton, MR (2009) Nature 458 :719. Nomenclature. Carcinoma Sarcoma Myeloma Leukaemia Lymphoma Melanoma

E N D
Hallmarks of Cancer Ellie Seaby
What is cancer? • “All cancers arise as a result of changes that have occurred in the DNA sequence of the genomes of cancer cells” • Stratton, MR (2009) Nature458:719
Nomenclature • Carcinoma • Sarcoma • Myeloma • Leukaemia • Lymphoma • Melanoma • “oma” vs “sarcoma” i.e. chondroma/chondrosarcoma
Benign vs Malignant • Tumours can be benign or malignant • Benign: NOT cancer • Benign: Incapable of invasion and metastasis • Benign: Can be as serious as malignant • Can benign become malignant?
Oncogenes • Oncogenes: Mutated proto-oncogenes that drive cell survival and proliferation i.e. Ras, HER2, VEGF Oncogenes are AUTOSOMAL DOMINANT!
Tumour suppressor genes • Tumour suppressor genes: encode proteins that normally slow down cell division, repair DNA mistakes, and trigger apoptosis. Inactivation of tumour suppressor genes can lead to cells growing out of control, which can lead to cancer.i.e. TP53, Rb, APC • Autosomal recessive!!
IN CANCER • Oncogenes are ACTIVATED • Tumour suppressor genes are INACTIVATED
Cancer mutations • Somatic: acquisition of mutations that convert a normal cell to a cancer cell • Germline: inheritance of an alteration or mutation that will cause or predispose to cancer i.e. Rb gene, APC (born with one defective copy - two-hit hypothesis)
Insensitivity to growth inhibitors Rb pRb is a TSG that controls progression through G1 checkpoint. If mutated cell can’t respond to anti-growth signals. Example: HPV interferes with Rb.
Avoiding apoptosis 50% of cancers have P53 mutations! Ignore the rest, remember this!
Limitless replicative potential • Most normal human cells have a capacity of 60-70 doubling, after the cell will enter non replicative senescence (G0) & result in shortening of telomeresat the end of chromosome • TOLEMERASE maintains chromosome length • 85-95% of cancer have up regulation of enzyme telomerase
Sustained angiogenesis • VEGF – neovasculatisation • Necrotic core • p53 inhibits VEGF – more blood vascularisation! • Bevacizumab (Avastin)
Tissue invasion & metastasis • Cells are held together by cellular adhesion molecules (CAMs) such as cadherins • E- cadherin is important in zonaadherens junctions. • E- cadherin function is lost and cells become “fibroblast” like able to invade the BM. • Integrins connect cells to ECM – loss of function = migration
Carcinogenesis of the bowel • APCRAS18qp53
Colon cancer screening – yes or no?! • About one in 20 people in the UK will develop bowel cancer during their lifetime. • It is the third most common cancer in the UK, and the second leading cause of cancer deaths, with over 16,000 people dying from it each year. • Regular bowel cancer screening has been shown to reduce the risk of dying from bowel cancer by 16 per cent.
Screening – Wilson and Jungner • the condition should be an important health problem • the natural history of the condition should be understood • there should be a recognisable latent or early symptomatic stage • there should be a test that is easy to perform and interpret, acceptable, accurate, reliable, sensitive and specific • there should be an accepted treatment recognised for the disease • treatment should be more effective if started early • there should be a policy on who should be treated • diagnosis and treatment should be cost-effective • case-finding should be a continuous process
UK Screening Programme • Every two years to all men and women aged 60 to 69. • Uses FOB (Faecal Occult Blood) kit sent in the post • Yes, you send your shit in the post! • High sensitivity • Low specificity • Positive tests referred for colonoscopy