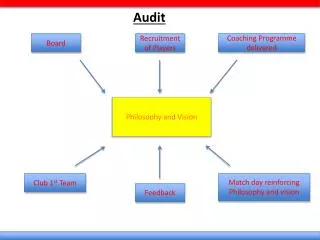
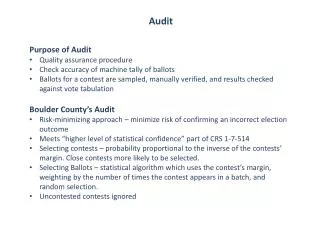
Audit
Audit. “ a critical systematic analysis of the quality of medical care – including outcomes use of resources and quality of life for the patient”. BASILDON ANTICOAGULANT SERVICE Consultant and Clinical Assistants seeing patients in clinic Prothrombin time measured by MLSO x 2

Audit
E N D
Presentation Transcript
Audit “ a critical systematic analysis of the quality of medical care – including outcomes use of resources and quality of life for the patient”
BASILDON ANTICOAGULANT SERVICE • Consultant and Clinical Assistants seeing patients in clinic Prothrombin time measured by MLSO x 2 • 600 patients – 3 weekly clinics • In control - 50% • No patient selection or education
BASILDON ANTICOAGULANT SERVICE 2002 Nurses see the patient in clinic, on ward and at home Automated analyser interfaced to computer NPT as required 2,400 patients New patients seen, others by request
Benchmarking exercises If same algorithm - what makes the difference ? Manual intervention Patient selection
% Time in Range Comparison for April 2002 Run, Site 11 and Range 2.50 % Time in Range This chart shows the time in range for all sites in ascending order. The bar below the line shows the time below range; the bar above the line shows the time above range. Your site is highlighted in red. The numbers of patients for each site are shown at the bottom of the chart.
PATIENT SELECTION The ideal patient: is co-operative can read has no other illnesses or drugs remembers what you tell them doesn’t worry is stable and temperate in their habits
Patient selection SPAF, etc. highly selective Beyth – multi-component intervention – 9% of older patients randomised Can we generalise from such a selected group?
RISK FACTORS FOR THROMBOSIS IN AF – SPAF 3 independent clinical predictors RR CCF 2.6 Multivarate Hypertension 2.2 PH of thrombo embolism 2.1 Event rate - % pa Age < 60 5.7 Univariate 61-75 5.9 > 75 8.0 Age as a multivariate risk feature RR = 1.2
RISK FACTORS FOR VTE Cancer 31% CCF 24% Fracture 10% MI 8% Obesity 4%
600 500 400 300 200 100 0 Male Patients Female Patients Incidence rate per 100,000 0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 >80 Age years
Evidence based medicine Like teenage sex The results are sometimes embarrassing Everyone thinks everyone else is doing it Those doing it have enthusiasm rather than expertise Old people disapprove of it
THE EVIDENCE BASE INCEPTION-COHORT PROSPECTVE COLLABORATIVE STUDY ITALIAN STUDY ON COMPLICATIONS OF ORAL ANTICOAGULANT TREATMENT (ISCOAT) Palaretti Lancet 1996 348 p423-8 2745 patients in 34 clinics followed for one year AGE < 70 1779 AGE > 70 966 Died 102 Died AC comp. 5
ANTICOAGULANT CONTROL 51566 INRs Mean interval 15 days Multivarcate Risk Ratios All ranges % control below above All patients 68 26 6 141 patients with bleeding 66 24 10 RR Relative Risk Factors age > 70 1.70 arterial disease 1.7 INR > 4.5 6 Timing – 1st 90 days 2.5
STUDY OBJECTIVES • To identify complication of anticoagulant therapy • As a basis for improved practice – • cf published works • To identify patients who would benefit from other treatments
Study Methods Review of 1 year’s patients –2,400 1/4/01 – 31/3/02 search of PAS for events • Bleeding + thromboses according to ICD codes Thrombosis DVT,PE TIA Search of blood bank needs for episodes GP + FHSA records for conformation/missing patients
Basildon results L I H Target on DAWN 32 1 1 Thromboses 5 Bleeds 22 2 5 INR on admission 29/39
INR for complications >12
Outcome: Recovered and continued warfarin 85% Recovered and stopped 9% Died 6% Death related to AC 0%
Co-morbidities Cancer 18% Arthritis 3% Heart failure – not stated
Local cause: Yes 29% Peptic ulcer 6% Ca. Colon 3% Bladder lesion 6% Bronchitis 3% Ca. Bronchus 6%
INTERACTING DRUGS Yes 32% Simvastatin 15% Aspirin 10% Amioderone 6% Diclofenac 3% Prednisolone 3%
ANTICOAGULANT CONTROL % in control below above All ranges ISCOAT 68 26 6 Basildon 67 22 11
INCIDENCE OF BLEEDING P.A. Fatal % Major %Minor % Levin – experimental studies ’92 0.4 2.4 8.5 Londfield review of similar studies ’93 0.8 4.9 15 Palaretti – prospective cohort study ’96 0.25 1.1 6.2 Watts + Clark retrospective 2002 0.0 0.6
Have we captured all the events ? Do clinicians report events to us ? Review of patients terminated in study period = 252 No. who have had blood transfusions = 13 2 Haemorrhagic deaths G.U. warfarin stopped 3/12 prior to fatal bleed post-op switched to IV heparin
PAS identifies admission and ICD code • PAS identifies death • Out of hospital death not necessarily referred • ? Outcomes • Check GP records • FHSA statistics
Follow-up of DNAs All DNAs get a reminder letter If 3 DNAs – letter from EJW to patient and GP 35 patient disappeared 10 ‘disappeared’ patients attended post 1.4.02 i.e. persistent poor attendees
What can DAWN tell us about our worst patients ? • Worst – out of range 90% of the time • 197 results from 24 patients • i.e. 1% of our patient population provide the 10% worst results • Improve patient selection Palaretti changed 11% to anti-platelet R, Basildon < 1%
What should we do with the Awkward Squad ? Educate Stop warfarin – alternatives aspirin aspirin + dipyridamole New R, pentasachoride DTIs Agatroban Ximelagatran Clinical review and explain risks of stopping ? Give all patients an annual review
Fibrinogen Melagatran (429,5 Da) Thrombin exosite 1 (fibrinogen) exosite 2 (heparin) active site
NEWER ANTITHROMBOTICS WILL BE EXPENSIVE They will be cost effect for : Housebound patients Poorly controlled patients Patients on interacting drugs ? Discharge to GP now
CONCLUSION : This audit has shown a lower incidence of major and fatal bleeding than in previously reported studies. The retrospective nature of the data collection means some cases of non-fatal bleeding and some thromboses may not have been identified. Robust systems of data capture are required Fatal episodes can be identified through FHSA records
Technological Trends INTERNET World-wide Intranet or “NHSnet” Computer Telephony Notebooks Telemedicine Web Enabled TV Video Voice Image Palmtops Mobile Phones
PCGs GPs Pharmacies Community e.g.Nurses Dentists Acute Hospitals A Possible New Model NHSNet or IntraNet Dawn AC Web Edition Security 24 hours Modem Browser Features Admin Needs a link for audit data collection
BASILDON ANTICOAGULANT SERVICE ? 2003 as 2002 + all patients to have (or be offered) a clinical review patients treated inappropriately to be terminated problems patients to be offered alternative R,