Download

1 / 112
1.13k likes | 1.28k Vues
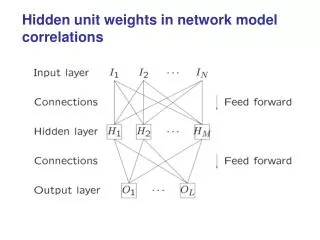
Targeting the HER2 network: what’s new?. P Pronzato, Genova. Increased cell proliferation Increased cell migration Resistance to apoptosis. HER2 Overexpression Leads to Increased Signaling. Yarden et al. Nat Rev Mol Cell Biol 2001. HER2 testing.

E N D
Targeting the HER2 network:what’s new? P Pronzato, Genova
Increased cell proliferation Increased cell migration Resistance to apoptosis HER2 Overexpression Leads to Increased Signaling Yarden et al. Nat Rev Mol Cell Biol 2001
In a randomized trial, benefit confined to HER2/neu amplified/overexpressors (Seidman, CALGB 9840) Subset analysis of CALGB 9840 suggests benefit in FISH-negative patients with Chr 17 2.2 (polysomy) (Kaufman, ASCO 2007) Trastuzumab and HER2 Status in Advanced Breast Cancer: Prior Observations R Livingston, ASCO 2008
Kaplan-Meier Estimates of PFS: HER2-Negative Subjects 1.0 Polysomy 17 ≤ 2.2, L+P (n = 178) Polysomy 17 > 2.2, L+P (n = 23) 0.8 Polysomy 17 ≤ 2.2, P (n = 183) Polysomy 17 > 2.2, P (n = 21) 0.6 Cumulative progression-free survival 0.4 0.2 0 0 20 40 60 80 100 120 Time, weeks
Benefit from adjuvant trastuzumab may not be confined to patients with IHC3+ and/or FISH positive tumors Paik et. Al, ASCO 2007, abstr. 511
Benefit from adjuvant trastuzumab may not be confined to patients with IHC3+ and/or FISH positive tumors Paik et. Al, ASCO 2007, abstr. 511
Benefit from adjuvant trastuzumab may not be confined to patients with IHC3+ and/or FISH positive tumors Paik et. Al, ASCO 2007, abstr. 511
ECD JC Thery
EGF30001 Study Design N = 579 • Key Inclusion • Incurable stage III/IV • No prior treatment for M+ • HER2-negative or untested RANDOMIZATION Paclitaxel 175 mg/m2 q3wLapatinib 1,500 mg PO QD (N = 291) • Stratification • Disease sites • Stage of disease Paclitaxel 175 mg/m2 q3w Placebo PO QD(N = 288) • Endpoints • Primary: TTP • Secondary: PFS, OS, safety Serum ECD measured by ELISA (Oncogene Science) pretreatment, week 9, and q12 weeks. Di Leo et al. J Clin Oncol. 2008. In press.
Poor Correlation of Baseline ECD With HER2 Status by FISH or IHC R = 0.34 (P< 0.001; n = 461) R = 0.28 overall (P < 0.001;n = 402)* *FISH+: R = 0.34 (P = 0.003; n = 75) FISH–: R = 0.03 (P = 0.596; n = 327) Correlation with IHC3+ 47/64 = 73%
Conversion From ECD-negative to -positive Is Associated With Worse PFS in HER2-negative Patients 1.0 1.0 0.8 0.8 P + Lapatinib P + Placebo 0.6 0.6 Converting Converting PFS PFS Non-converting (remain negative) Non-converting (remain negative) 0.4 0.4 0.2 0.2 0.0 0.0 0 20 40 60 80 100 120 0 20 40 60 80 100 120 Time, weeks Time, weeks HR = Hazard of converting.
Conversion From ECD-positive to -negative Is Associated With Improved PFS 1.0 1.0 0.8 0.8 P + Lapatinib P + Placebo 0.6 0.6 Converting Converting PFS PFS Non-converting (remain positive) Non-converting (remain positive) 0.4 0.4 0.2 0.2 0.0 0.0 0 20 40 60 80 100 120 0 20 40 60 80 100 120 Time, weeks Time, weeks HR = Hazard of converting. 30 patients seroconvertered: 17 PR, 12 SD, 1 PD
Study Design • arm A: trastuzumab (T) + docetaxel (D) (100mg/m2, q3wks), • with continuation of T after D until PD • R • arm B: trastuzumab docetaxel (100mg/m2, q3wks) • at PD • loading dose trastuzumab 4 mg/kg, thereafter weekly 2 mg/kg • docetaxel: at least 6 cycles • no routine use of haematological growth factor support
Best Overall Response during treatment (RECIST criteria) Combination Sequential T + D T H p = 0.03
Median time to first progression p=0.0001 Combination therapy T + D: 9.4 mo Monotherapy T : 3.9 mo
Progression Free SurvivalCombination versus Sequential therapy p=0.42 Combination T + D: 9.4 mo Sequential T D: 10.8 mo
Overall Survival Combination T + D: 30.5 mo Sequential T D: 20.2 mo p=0.15
Herceptin prolongs survival in women with 1st-line MBC H0648g (IHC 3+) M77001 BCIRG 007 US Oncology (IHC 3+) Median survival (months) IHC, immunohistochemistry; P, paclitaxel H, Herceptin; D, docetaxel; Carbo, carboplatin Smith et al 2001; Marty et al 2005 Robert et al 2006; Pegram et al 2007
HTX Herceptin 8mg/kg (loading dose), d1followed by 6mg/kg, d1, q21d Docetaxel 75mg/m2, d1 Xeloda 950mg/m2 bid, d1–14 R A N D O M I S A T I O N HT Herceptin 8mg/kg (loading dose), d1 followed by 6mg/kg, d1, q21d Docetaxel 100mg/m2, d1 CHAT: a large randomised phase II trial No prior Herceptin, docetaxel or Xeloda • Stratification: • prior paclitaxel • prior anthracycline • liver metastases • KPS KPS = Karnofsky performance status Wardley A et al. Breast Cancer Res Treat 2007;106(Suppl. 1):S33(Abst 309)
HTX significantly increases progression-free survival Events HR 95% CI p-value HTX 75 0.725 0.529, 0.99 0.0402 HT 85 1.0 0.8 0.6 0.4 0.2 0 Estimated probability 12.8 17.9 0 5 10 15 20 25 30 35 40 45 50 Months Wardley A et al. Breast Cancer Res Treat 2007;106(Suppl. 1):S33(Abst 309)
Phase III Study to Test if Total HER2 Blockade Improves Clinical Outcome RANDOMIZATION • Key Inclusion • HER2+(FISH+/ IHC3+) MBC • Progression on • Anthracycline • Taxane • Trastuzumab • Progression on most recent trastuzumab regimen Lapatinib 1500 mg/day PO N=148 Crossover if PD after 4wk therapy (N=73) • Stratification Factors • Visceral Disease • Hormone Receptor Lapatinib 1000 mg/day PO Trastuzumab 4 2 mg/kg IV qw N=148 J O Shaughnessy, ASCO 2008 Study conducted and funded by GlaxoSmithKline
Treatment Efficacy *Confirmed CR+PR †CR+PR+SD ≥ 6 mo
Progression-Free Survival 100 80 60 Cumulative % Alive without Progression 40 28% 6 Mo PFS 20 13% 0 0 10 20 30 40 50 60 Time from Randomization (wks) Subjects At Risk L L+T 148 148 53 73 21 42 13 27 5 8 0 2
Adjuvant Herceptin has an extensive evidence base with >13,000 patients treated in 4 major trials Docetaxel + carboplatin Docetaxel Herceptin Paclitaxel Standard CTx HERA (ex-USA) BCIRG 006 (global) Observation IHC / FISH (n=5,090) FISH(n=3,222) 1 year 1 year 2 years 1 year NCCTG N9831 (USA) NSABP B-31 (USA) IHC / FISH (n=2,030) IHC / FISH (n=3,505) 1 year 1 year 1 year Doxorubicin + cyclophosphamide IHC, immunohistochemistry FISH, fluorescence in situ hybridisation CTx, chemotherapy Piccart-Gebhart et al 2005 Romond et al 2005; Slamon et al 2006
HERA HERA update Lancet 2007
1 In favor of Obs. Trastuzumab Adjuvant Trials 0 2 In favor of T