Pediatric Stroke
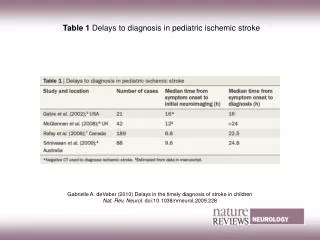
Pediatric Stroke. Last Updated by Lindsay Pagano Summer 2013. Epidemiology of Childhood Stroke. *Incidence rate is per 100,000 child-years Overall, childhood stroke is as common as brain tumor in childhood !! Numbers from: Fullerton et al. Neurology 2003. Signs, Symptoms and Differential.

Pediatric Stroke
E N D
Presentation Transcript
Pediatric Stroke Last Updated by Lindsay Pagano Summer 2013
Epidemiology of Childhood Stroke • *Incidence rate is per 100,000 child-years • Overall, childhood stroke is as common as brain tumor in childhood !! • Numbers from: Fullerton et al. Neurology 2003.
Signs, Symptoms and Differential Symptoms/Signs • Hemiparesis/focal motor 60% • Aphasia 10-15% • Seizure 25% (vs. 5% in adults) • Headache 32% • Altered mental status 21% Differential • Complex Migraine: eg focal aura, hemiplegic migraine • Focal seizure with postictal focal weakness (Todd’s paralysis/plegia) • Stroke – Ischemic/Hemorrhagic • Other focal brain pathology • Stroke Mimics can include: • Encephalopathy related to hypertension, intracranial infection, tumor, drug toxicity, pseudotumorcerebri, inflammatory disease, epilepsy
Etiology of Ischemic Stroke in Older Kids: Think Embolic or Arteriopathy • Arteriopathy – present in 60-80% of Children • Arterial Dissection in 25% , also Focal cerebral arteriopathy, Moyamoya, post-infectious, HIV, Varicella, etc. • Cardioembolism 25-35% • Sickle Cell Anemia • 10% will have a clinical stroke by age 20 • 20% more will have a silent infarct • Hypercoaguable state • More unusual causes: vasculitis, pregnancy, metabolic disorders, cerebral sinus venous thrombosis • Idiopathic 5-30%
Acute Management of Child with Possible Stroke: The First 15 Minutes! Goals: 1. cerebral perfusion 2. oxygenation 3. minimize demands for cerebral blood flow • Head of Bed Flat –if alert, or 30 degrees if not alert/aspiration risk. • IV Fluids: isotonic, at maintenance+, no dextrose – as want to avoid hyperglycemia. Check sugars • Oxygen only if needed to keep sats > 95% • Acetaminophen if temp > 37.0 • Get a neuro exam you can follow serially • Peds NIHSS- Peds Stroke Cards
Diagnostic Evaluation Ischemic Stroke: Head, Neck, Heart, Blood Acutely • MRIbrain, MRA head,neck • At VCH: Order emergentpeds stroke protocol brain MRI in all kids with symptoms < 48 hours or if stroke will change management dramatically • Protocol takes 10 minutes and includes: • DWI bright and ADC dark = acute stroke (within the last 10 days) • FFE/GRE: sequence for blood • No MRA if MRI shows stroke • +/- MR Venogram (especially consider with sickle cell disease) • Note: Head CT will miss 60% of acute stroke within 12 hours of symptom onset. Need MRI. • Note: Neck vessel imaging - MR or CT Angiography, NOT ultrasound After initial head imaging • Echo – Transthoracic Echo with bubble study to eval for PFO, thrombus source • Coagulation evaluation
Treatment Aspirin • For all older children with ischemic stroke except kids with sickle cell disease • Typical dose is 3-5 mg/kg/day • Risk of Reye’s syndrome is very low. Still we strongly recommend annual flu vaccine and some will hold aspirin with high fever or flu-like symptoms (I don’t). Anticoagulation • Consider if suspicion high for cardioembolic stroke, arterial dissection, posterior circulation stroke, stuttering deficits suggestive of thrombosis. • Risk of hemorrhagic transformation of ischemic stroke is less after 48 hours. • May prevent further strokes, but won’t help this one improve. **Sickle Cell Disease/HbSS • Treatment is Transfusion (usually, pRBC in ED, exchange transfusion in PICU) • Regular transfusions through heme/onc as indicated in the future
PREP Question A 6 year old right handed girl with no significant past medical history presents to the emergency department for concerns of new onset right sided weakness that was first noted when she tried to get out of bed that morning. Her speech was also slurred. Her symptoms seemed to improve throughout the morning but did not completely resolve. There were no witnessed convulsions or associated loss of consciousness. Her birth history was uncomplicated, and her development has been appropriate. PE is significant for slurred speech with short sentences, difficulty following commands, and flattening of the right nasolabial fold. She also has a slight decrease in right sided tone and 4/5 strength on the right. There is a right plantar extensor response. Of the following, the MOST accurate statement is: A. The most likely vascular territory involved is the right middle cerebral artery. B. The most likely lesion producing these symptoms is one involving the left internal capsule. C. Angiogram could show abnormal collateral arterial networks. D. The most likely diagnosis is complicated migraine, and the family can be reassured and the patient discharged. E. The best characterization of her speech deficit is dysarthria.
C. Angiogram could show abnormal collateral arterial networks MoyamoyaVasculopathy • Idiopathic versus associated with other disease states • NF1, fibromuscular dysplasia, Marfan syndrome, Down syndrome, radiation vasculitis, vasculitis, infectious/postinfectiousvasculopathy, congenital heart disease, sickle cell disease, Fanconi anemia, atherosclerosis, head trauma • Noninflammatory, progressive cerebrovascular occlusive disease slowly causing stenosis and occlusion of cerebral arteries, especially those surrounding or feeding the Circle of Willis • “puff of smoke” • Regarding the other choices: A. The most likely vascular territory involved is the right MCA: left MCA is most likely since she is right handed, and her cortical language and left motor areas are involved B. The most likely lesion producing these symptoms is one involving the right internal capsule: as above D. The most likely diagnosis is complicated migraine, and the family can be reassured and the patient discharged: this may be the diagnosis, but need to rule out acute stroke E. The best characterization of her speech deficit is dysarthria: dysarthria AND aphasia (both receptive and expressive)